目的 探讨动态对比增强磁共振(DCE-MRI) 在界定脑胶质瘤病理级别中的诊断价值。方法 回顾分析南阳市第二人民医院2014-11—2016-09经临床或者病理证实为脑胶质瘤患者39例,男25例,女14例,年龄14~70(46±12)岁。病理分级Ⅱ级19例,Ⅲ级11例,Ⅳ级 9例。采用免疫组化的方法对每例手术样本进行CD105-微血管密度 (CD105-MVD)检测。采用Mann-Whitney U-test对不同级别胶质瘤的Ktrans、Ve 和CD105-MVD 进行差别验证。采用Pearman相
动态对比增强磁共振在脑胶质瘤病理级别中的诊断价值
李运奇1) 尹先哲2) 汤 韬2) 赵智伟3)△
1)南阳市第二人民医院医学影像科,河南 南阳 473012 2)南阳市第二人民医院神经外科,河南 南阳 473012 3)河南科技大学第一附属医院康复科,河南 洛阳 471000
基金项目:河南省医学科技攻关计划项目(201602378)
作者简介:李运奇,Email:584091813@qq.com
△通信作者:赵智伟,Email:zhaozhiwei1980@sina.com
【摘要】 目的 探讨动态对比增强磁共振(DCE-MRI) 在界定脑胶质瘤病理级别中的诊断价值。方法 回顾分析南阳市第二人民医院2014-11—2016-09经临床或者病理证实为脑胶质瘤患者39例,男25例,女14例,年龄14~70(46±12)岁。病理分级Ⅱ级19例,Ⅲ级11例,Ⅳ级 9例。采用免疫组化的方法对每例手术样本进行CD105-微血管密度 (CD105-MVD)检测。采用Mann-Whitney U-test对不同级别胶质瘤的Ktrans、Ve 和CD105-MVD 进行差别验证。采用Pearman相关性分析 Ktrans和 Ve 与CD105-MVD的相关性。结果 Ktrans、Ve和CD105-MVD在低级神经胶质瘤(LGG)和高级神经胶质瘤(HGG)之间有显著的统计学差异(P=0.001、P<0.001、P<0.001)。病理分级Ⅱ级的Ktrans、Ve和CD105-MVD明显低于Ⅲ级和Ⅳ级。在高级别胶质瘤中Ktrans与CD105-MVD,Ve与CD105-MVD均呈正相关(P<0.001、P<0.001)。结论 DCE-MRI在无创评估部分神经胶质瘤的MVD中具有一定的作用,值得普及。
【关键词】 胶质瘤;动态对比增强磁共振;CD105-MVD;诊断;病理分级
【中图分类号】 R739.41 【文献标识码】 A 【文章编号】 1673-5110(2018)13-1407-06 DOI:10.12083/SYSJ.2018.13.332
The value of dynamic contrast enhanced MRI in the diagnosis of glioma pathology
LI Yunqi1),YIN Xianzhe2),TANG Tao2),ZHAO Zhiwei3)
1)Department of Imaging,the Second People's Hospital of Nanyang,Nanyang 473000,China;2)Department of Neurosurgery,the Second People's Hospital of Nanyang,Nanyang 473000,China;3)Department of Rehabilitation,First Affiliated Hospital of Henan University of Science and Technology,Luoyang 471000,China
【Abstract】 Objective To discusses and analyze the value of dynamic contrast-enhanced (DCE) MRI in the glioma pathology diagnosis.Methods We retrospective analyzed the 39 glioma patients diagnosed by clinical or pathological methods from November 2014 to September 2016.By using immunohistochemical method,we tested the CD105-microvascular density (CD105-MVD) for 39 operation samples.By using the Mann-Whitney U-test,we analyzed the different of Ktrans,Ve and CD105-MVD between different grade gliomas.By using Pearman correlation analysis,we analyzed the correlation of Ktrans,Ve and CD105-MVD.Results The differences were statistically significant in Ktrans,Ve and CD105-MVD between low-grade gliomas (LGG) and high-grade glioma (HGG) (P=0.001,P<0.001,P<0.001).Ktrans,Ve and CD105-MVD of pathology classification Ⅱ level significantly lower than the level Ⅲ and Ⅳ.Ktrans,Ve and CD105-MVD were positively correlated in the HGG (P<0.001,P<0.001).Conclusion Our research results show that the DCE-MRI plays an important role in noninvasive evaluation in part of the MVD of the glioma,and worthy of popularizing.
【Key words】 Glioma;DCE-MRI;CD105-MVD;Diagnose;Pathology classification
微血管增生是脑胶质瘤一个重要的组织学特征[1-2]。神经胶质瘤微血管通透性在预测病理分级、预后有重要意义[3]。病理分级不同的神经胶质瘤微血管增生的程度不同[4-5]。然而,采用免疫组织化学技术检测CD105-MVD需要手术或活检标本,这可能会导致脑组织损伤和抽样误差。动态对比增强磁共振成像(DCEMRI)可以通过分析对比剂分子通过的程度无创评估神经胶质瘤不成熟的微血管的通透性。本文研究DCE-MRI与CD105-MVD水平的关系,探讨论在神经胶质瘤中是否可以以非侵入性的方式(如DCE-MRI)评估MVD的程度。
1 资料与方法
1.1 一般资料 选取回顾分析南阳市第二人民医院2014-11—2016-09经临床或者病理证实为脑胶质瘤患者39例,诊断根据2016年世界卫生组织(WHO)分类进行[6]。男25例,女14例,年龄14~70(46±12)岁。病理分级Ⅱ级19例,Ⅲ级11例,Ⅳ级 9例。在接受DCE-MRI检查之前,所有患者均未接受任何颅内手术、化疗或者放疗等治疗。
1.2 方法 选择西门子3.0T超导MR仪,头部正交线圈,对全部患者实施MRI平扫横断和冠状、矢状扫描。扫描参数,DCE-MRI使用以下执行序列:强化前数据集的获得采用T1WI作为基线(TR/TE,5.1/1.8 ms;视场角(FOV)240 mm×240 mm;矩阵138×192;扫描厚度、3.6mm),翻转角度2°和15°。DCE信号收集(TR/TE,4.9/1.9 ms;FOV,240 mm×240 mm;矩阵,138×192;扫描厚度3.6 mm),翻转角度12°,测量时间间隔为4.29 s。第五个基线数据获得后,通过肘前静脉注射钆双胺注射液(Gd-DTPA-BMA;欧乃影,通用电气医疗集团,挪威),注射剂量为0.1 mmol/kg,速度4 mL/s。
1.3 数据分析 所有数据传入Siemens工作站,采用血流动力学模型获得脑组织的时间—信号强度曲线。采用Tofts和Kermode药代动力学模型计算Ktrans和Ve。通过颈内动脉段信号强度的变化得到动脉输入函数。通过同步观测在轴向对比度T1WI成像和相应的Ktrans和Ve参数图确定Ktrans和Ve值。 ROIs区域被自动转移到轴向对比度T1WI成像和Ktrans和Ve参数图中。每个肿瘤的ROI大小保持不变(半径4~6 mm)。每个病人测量3次ROIs,选择三次中Ktrans和Ve最大值。 ROI由神经系统放射人员手工绘制。避开ROIs区域中的囊性坏死,出血区域和正常的微血管区域。
1.4 免疫组化染色和诊断 39例胶质瘤组织样本全部经10%甲醛溶液固定,石蜡包埋,切成4 μm厚的组织切片。CD105兔多克隆抗体(Abcam,美国)作为一抗对MVD进行检测评估,采用链霉菌抗生物素过氧化酶(SP)免疫组化法对切片进行染色。显微镜下观察组织切片染色情况,并应用显微摄像系统进行图像采集。病理诊断根据2016年WHO分类标准进行。以阳性对照片和PBS代替一抗的阴性对照片进行对照。阳性切片的判断:微血管出现棕黄色颗粒为染色阳性。用光密度值(OD)表示阳性细胞表达情况。OD值=整合的光密度/构成对象的像素数。
1.5 统计学处理 所得数据采用SPSS 14.0软件进行统计分析,计量资料以(x±s)表示,采用Mann-Whitney U-test对不同级别胶质瘤的Ktrans、Ve 和CD105-MVD 进行差别验证。采用Pearman相关性分析 Ktrans、 Ve和 CD105-MVD的相关性。以P<0.05为差异有统计学意义。
2 结果
2.1 Ktrans、 Ve和 CD105-MVD与胶质瘤病理分级的关系 低级别胶质瘤(LGG)和高级别胶质瘤(HGG)的平均Ktrans、Ve、CD105-MVD值如表1所示。LGG的Ktrans和Ve明显低于HGG (P=0.001,P<0.001)。LGG的CD105-MVD明显低于HGG(P<0.001)。Ⅲ级与Ⅳ级Ktrans、Ve和CD105-MVD无明显差异。
表1 Ktrans、 Ve和 CD105-MVD与胶质瘤病理分级的关系
Table 1 Relationship between Ktrans,Ve and cd105-mvd and the pathological grade of glioma
| 参数 |
G2 |
G3 |
G4 |
G3+G4 |
| Ktrans |
0.039±0.033 |
0.123±0.034 |
0.160±0.131 |
0.132±0.107 |
| Ve(no units) |
0.109±0.156 |
0.323±0.145 |
0.361±0.216 |
0.353±0.226 |
| CD105-MVD(%) |
0.710±0.220 |
1.805±0.704 |
2.120±0.931 |
1.905±0.923 |
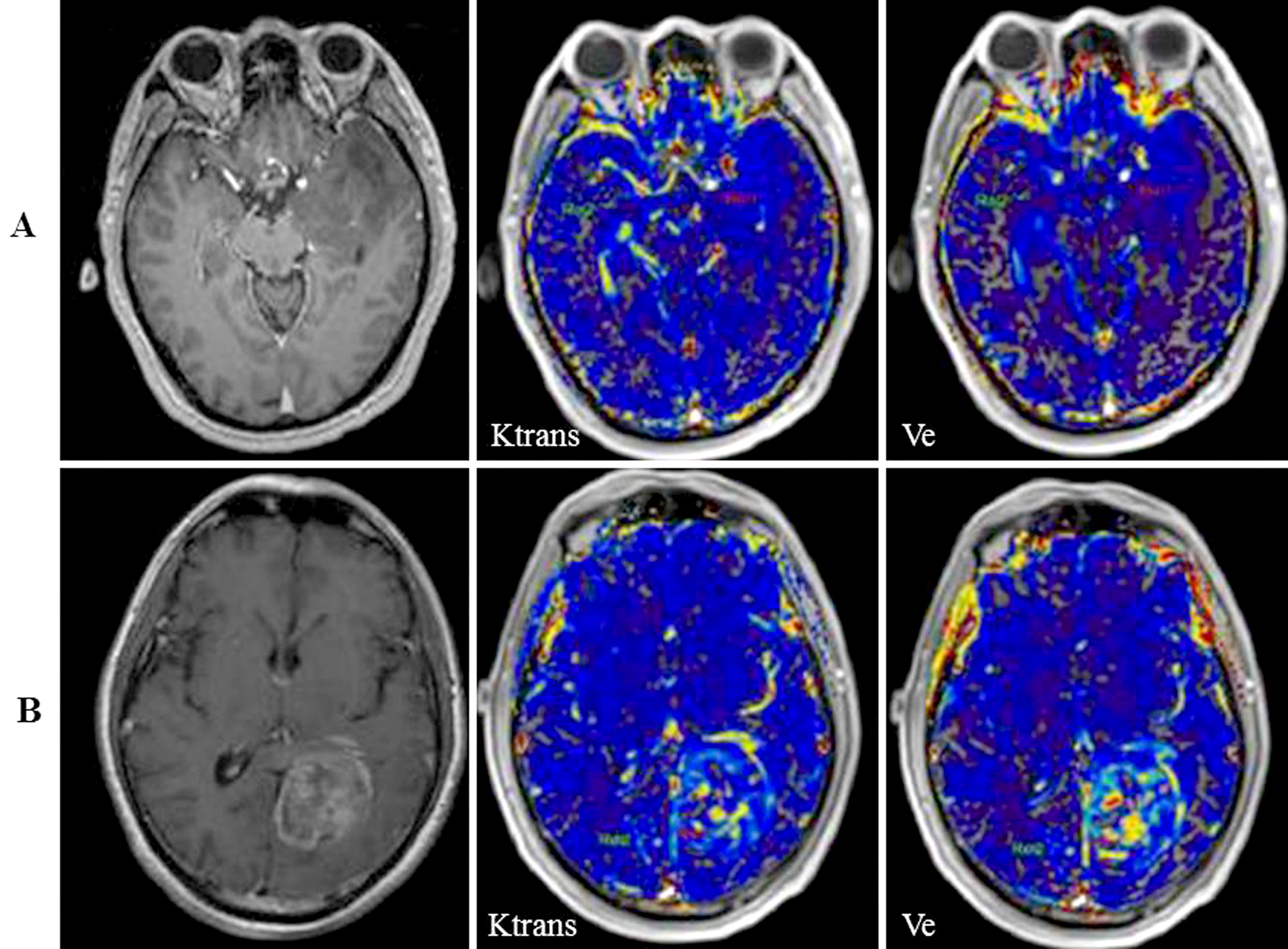
2.2 神经胶质瘤中Ktrans、Ve 和CD105-MVD之间的相关分析 在高病理级别的胶质瘤(HGG)中Ktrans和Ve都与CD105-MVD呈正相关(r=0.698,P<0.001;r=0.682,P<0.001)。而低病理级别的胶质瘤(LGG)中Ktrans和Ve与CD105-MVD无明显相关性(图1)。
图1 低级别胶质瘤和高级别胶质瘤MRI影像图比较。A组从左到右依次为:病理级别Ⅱ级的胶质瘤MRI (T1WI) 影像图,Ktrans影像图,Ve影像图;B组从左到右依次为:病理级别Ⅳ级的胶质瘤MRI (T1WI) 影像图、Ktrans影像图、Ve影像图
Figure 1 Comparison of MRI images of low grade glioma and high grade glioma.A group from left to right in turn:on the left side of the level of pathological Ⅱ grade of glioma MRI images of (T1WI),images of Ktrans,Ve image;In group B,from left to right,the left pathological grade IV glioma MRI (T1WI) image,Ktranss image and Ve image were successively shown
3 讨论
肿瘤血管生成是神经胶质瘤发生和发展中一个关键的过程,该过程为肿瘤入侵健康组织提供了充足的氧和营养物质[7-9]。目前,越来越多的研究发现,基于MVD的组织学方法评价肿瘤血管生成是一个神经胶质瘤患者的独立预后指[10-14]。目前的一些标记物不能区分生理状态下和病理状态下的微血管增殖,如CD31[15-17]、CD34 [18-20]、CD3[21-24]、CD20[25-26]和凝血因子Ⅷ[4]。因此,这些标记物的免疫染色得出的MVD不能对微血管生成的程度提供一个准确的估计。CD105是一个共受体,属于TGF-beta家族,其表达与新生不成熟的微血管有关[12,27-28]。多项研究表明,CD105可能是一个特异的异常微血管生成标记[29-31]。 CD105阳性表示神经胶质瘤微血管程度高,肿瘤恶性程度高[32-34]。这些CD105阳性的微血管通透性大,这会增加血管内容物渗漏到血管外的组织间隙,为神经胶质瘤肿瘤细胞入侵正常组织提供了条件[35-37]。之前有研究已经确定,CD105在星形细胞瘤微血管内皮细胞中阳性表达,CD105-MVD的表达水平与神经胶质瘤病理的等级成正相关[10] 。本研究显示,LGG中CD105-MVD的表达水平明显低于HGG,HGG中的与肿瘤恶性程度相关的不成熟微血管可能会比LGG更多。Ⅲ和Ⅳ级神经胶质瘤之间的CD105-MVD的表达水平没有显著差异。这可能是由于这两个级别神经胶质瘤中的微血管增生程度类似。临床上检测并评估CD105-MVD的表达水平方法复杂且费用高。因此,无创性评CD105-MVD的表达情况从而间接得出不成熟微血管的增生和识别潜在的恶性神经胶质瘤意义非同一般。
这些初步结果可以作为进一步验证的基础。目前,该项研究还有诸多不足之处。在该项研究过程中,遇到了一些目前无法克服的问题,如DCE-MRI数据处理前需要提前得到动脉输入函数(arterial input function,AIF),AIF选择不同的动脉及其ROI选择位置是否合理,都将显著影响计算结果[38-39],从而无法准确评估组织微血管特性。最准确的AIF应该是目标区的直接供血动脉,但由于空间分辨率受限,常常无法观察到,因此常用扫描范围内的动脉代替[40]。另外AIF与被检者自身BMI指数、每搏输出量有关,因此个体化AIF是最佳选择,但其对时间分辨率要求较高,提高可重复性是临床应用的关键因素。时间分辨率、空间分辨率较低的情况下,考虑选择Reference模型或者Population AIF[41]。运动位移在DCE-MRI数据中普遍存在,如:头颈部,吞咽、舌头及下颚的活动;肺部及乳腺,呼吸运动、心脏跳动;肝、肾,胃肠蠕动等。AIF曲线由于血管运动不能够真正反映对比剂进人体内的全过程。病灶边缘由于运动位移模糊不清,直接影响病灶感兴趣区勾画,进而对拟合病灶时间一信号强度曲线的真实度及准确度产生误差[42-44]。因此,运动校准是很有必要的,校准每一个像素点的位置,以保证计算结果的可靠性。
由DCE-MRI 得到的Ktrans和Ve对评估神经胶质瘤微血管通透性来讲是一个非侵入性的理想的检测方式[45-48]。DCE-MRI已经证实HGG的微血管渗透率大于LGG[49]。本研究显示,LGG的 Ktrans和Ve值明显低于HGG。神经胶质瘤中不成熟的微血管通透性大,正常成熟的微血管内皮完整,血管内容无或分子的转移受到有效的限制。
本文显示,HGG中有更多的不成熟和高渗透性的微血管。但在异常的Ktrans或者Ve信号和病理标本中很难执行voxel-by-voxe对比。 因此,不能排除抽样误差所造成研究结果偏差的可能性。针对这一点我们假设高的trans和Ve信号代表高度不成熟的MVD脑部区域,其他区域依据于此进行比较。
另外在图像后期处理中,处理软件所采用都是标准化的模型,该模型简化了一些数据处理工作,不能很好的评估一些数据的有效性。 如在该项研究中,血管内的血清体积不能很好的被计算出来。采用合适的模型可能会更好地描述一些重要的生理参数和生物效应。但是不同肿瘤类型,肿瘤部位和治疗方法最适合的数据处理模型也不一样[50],因此我们只能采用目前被广泛认可的标准化模型来进行后期图像处理。该研究还必须要考虑到等离子体体积的影响,该种影响一般情况下可忽略不计。但是这种影响可能导致在0.05~0.10 mL/g血管等离子体体积的范围内Ktrans会被略高估值。另一个可能导致数值估偏的原因是基线ROI模版。比如,明显的肿瘤水肿或早期治疗失败,随着肿瘤组织体积的增加,最终得到的DCE-MRI图像可能无法真正的反映肿瘤增殖情况。本研究未观察到这种情况,然而,非线性注册方法,如弹性图像算法可以用于获取与串行成像研究相匹配的序列或。本研究的另一个局限是样本量相对较小,需要大规模的病例研究更客观地证实灌注量的估计和体内肿瘤状态之间的关系。
4 参考文献
[1] DIGERNES I,BJORNERUD A,VATNEHOL S A S,et al.A theoretical framework for determining cerebral vascular function and heterogeneity from dynamic susceptibility contrast MRI[J].J Cereb Blood Flow Metab,2017,37(6):2 237-2 248.
[2] HEILAND D H,DEMERATH T,KELLNER E,et al.Molecular differences between cerebral blood volume and vessel size in glioblastoma multiforme[J].Oncotarget,2017,8(7):11 083-11 093.
[3] SATO S,SATO Y,HATAKEYAMA K,et al.Quantitative analysis of vessels with smooth muscle layer in astrocytic tumors:correlation with histological grade and prognostic significance[J].Histol Histopathol,2011,26(4):497-504.
[4] YAO Y,KUBOTA T,TAKEUCHI H,et al.Prognostic significance of microvessel density determined by an anti-CD105/endoglin monoclonal antibody in astrocytic tumors:comparison with an anti-CD31 monoclonal antibody[J].Neuropathology,2005,25(3):201-206.
[5] SENGUPTA R,BARONE A,MARASA J,et al.Novel chemical library screen identifies naturally occurring plant products that specifically disrupt glioblastoma-endothelial cell interactions[J].Oncotarget,2015,6(21):18 282-18 292.
[6] BANAN R,HARTMANN C.The new WHO 2016 classification of brain tumors-what neurosurgeons need to know[J].Acta neurochirurgica,2017,159(3):403-418.
[7] WANG C,LI Y,CHEN H,et al.CYP4X1 Inhibition by Flavonoid CH625 Normalizes Glioma Vasculature through Reprogramming TAMs via CB2 and EGFR-STAT3 Axis[J].J Pharmacol Exp Ther,2018,365(1):72-83.
[8] DONG J,SAUNDERS D,SILASI-MANSAT R,et al.Therapeutic efficacy of a synthetic epsin mimetic peptide in glioma tumor model:uncovering multiple mechanisms beyond the VEGF-associated tumor angiogenesis[J].J Neurooncol,2018 Jan 22.doi:10.1007/s11060-018-2 766-z.
[9] SZABO E,PHILLIPS D J,DROSTE M,et al.Anti-tumor activity of DLX1008,an anti-VEGFA antibody fragment with low picomolar affinity,in human glioma models[J].J Pharmacol Exp Ther,2018Mar5.pii:jpet.117.246249.doi:10.1124/jpet.117.246249
[10] NETTO G C,BLEIL C B,HILBIG A,et al.Immunohistochemical evaluation of the microvascular density through the expression of TGF-beta (CD 105/endoglin) and CD 34 receptors and expression of the vascular endothelial growth factor (VEGF) in oligodendrogliomas[J].Neuropathology,2008,28(1):17-23.
[11] JIA Z Z,SHI W,SHI J L,et al.Comparison between perfusion computed tomography and dynamic contrast-enhanced magnetic resonance imaging in assessing glioblastoma microvasculature[J].Eur J Radiol,2017,87:120-124.
[12] JIA Z Z,GU H M,ZHOU X J,et al.The assessment of immature microvascular density in brain gliomas with dynamic contrast-enhanced magnetic resonance imaging[J].Eur J Radiol,2015,84(9):1 805-1 809.
[13] LU N,DI Y,FENG X Y,et al.CT perfusion with acetazolamide challenge in C6 gliomas and angiogenesis[J].PloS one,2015,10(3):e0 121 631.
[14] SICA G,LAMA G,ANILE C,et al.Assessment of angiogenesis by CD105 and nestin expression in peritumor tissue of glioblastoma[J].Int J Oncol,2011,38(1):41-49.
[15] SHAIK S,KENNIS B,MAEGAWA S,et al.REST upregulates gremlin to modulate diffuse intrinsic pontine glioma vasculature[J].Oncotarget,2018,9(4):5 233-5 250.
[16] HIRA V V,PLOEGMAKERS K J,GREVERS F,et al.CD133+ and Nestin+ Glioma Stem-Like Cells Reside Around CD31+ Arterioles in Niches that Express SDF-1alpha,CXCR4,Osteopontin and Cathepsin K[J].J Histochem Cytochem,2015,63(7):481-493.
[17] MUSUMECI G,CASTORINA A,MAGRO G,et al.Enhanced expression of CD31/platelet endothelial cell adhesion molecule 1 (PECAM1) correlates with hypoxia inducible factor-1 alpha (HIF-1alpha) in human glioblastoma multiforme[J].Exp Cell Res,2015,339(2):407-416.
[18] MAJCHRZAK K,KASPERA W,SZYMAS J,et al.Markers of angiogenesis (CD31,CD34,rCBV) and their prognostic value in low-grade gliomas[J].Neurol Neurochir Pol,2013,47(4):325-331.
[19] HUSE J T,SNUDERL M,JONES D T,et al.Polymorphous low-grade neuroepithelial tumor of the young (PLNTY):an epileptogenic neoplasm with oligodendroglioma-like components,aberrant CD34 expression,and genetic alterations involving the MAP kinase pathway[J].Acta Neuropathol,2017,133(3):417-429.
[20] DUAN S.Silencing the autophagy-specific gene Beclin-1 contributes to attenuated hypoxia-induced vascu-logenic mimicry formation in glioma[J].Cancer Biomark,2018,21(3):565-574.
[21] GEDEON P C,SCHALLER T H,CHITNENI S K.A rationally designed fully human EGFRvIII:CD3-targeted bispecific antibody redirects human T cells to treat patient-derived intracerebral malignant glioma[J].Clin Cancer Res,2018,27.doi:10.1158/1078-0432.CCR-17-0126.
[22] CHOI B D,KUAN C T,SURYADEVARA C M,et al.Tim-3 expression predicts the abnormal innate immune status and poor prognosis of glioma patients[J].Clin Chim Acta,2018,476:178-184.
[23] TEZER F I,FIRAT A,TUZUN E,et al.Immunopathology in drug resistant mesial temporal lobe epilepsy with different types of hippocampal sclerosis[J].Int J Neurosci,2018,128(5):421-428.
[24] WANG Y G,LONG J,SHAO D C,et al.Hyperbaric oxygen inhibits production of CD3+ T cells in the thymus and facilitates malignant glioma cell growth[J].J Int Med Res,2018,1:300060518767796.doi:10.1177/0300060518767796.
[25] RISSI D R,PORTER B F,BOUDREAU C E,et al.Immunohistochemical Characterization of Immune Cell Infiltration in Feline Glioma[J].J Comp Pathol,2018,160:15-22.
[26] SUZUKI A,MARUYAMA T,NITTA M,et al.Modified rapid immunohistochemical staining for intraoperative diagnosis of malignant brain tumors[J].Brain Tumor Pathol,2017,34(4):141-148.
[27] SMIRNOV I V,GRYAZEVA I V,SAMOILOVICH M P,et al.Endoglin (CD105)-a target for visualization and anti-angiogenic therapy for malignant tumors[J].Vopr Onkol,2015,61(6):898-907.
[28] ZHANG J,ZHANG L,LIN Q,et al.Prognostic value of endoglin-assessed microvessel density in cancer patients:a systematic review and meta-analysis[J].Oncotarget,2018,9(7):7 660-7 671.
[29] YILMAZ I,ERDOGAN U,TANRIVERDI O,et al.Evaluation of Bevacizumab for The Treatment of Epidural Fibrosis by Immunohistochemical Staining for CD105 and Osteopontin[J].Turk Neurosurg,2018 Feb 21.doi:10.5137/1019-5149.
[30] DAS L,NASKAR S,SARKAR T,et al.Immunohistochemical evaluation of prime molecules in cervical lesions towards assessment of malignant potentiality[J].J Cancer Res Ther,2018,14(2):377-381.
[31] ZHUO H,ZHENG B,LIU J,et al.Efficient targeted tumor imaging and secreted endostatin gene delivery by anti-CD105 immunoliposomes[J].J Exp Clin Cancer Res,2018,37(1):42-47.
[32] AFSHAR MOGHADDAM N,MAHSUNI P,TAHERI D.Evaluation of Endoglin as an Angiogenesis Marker in Glioblastoma[J].Iran J Pathol,2015,10(2):89-96.
[33] LIU Q,ZHANG R Z,LI D,et al.Muse Cells,a New Type of Pluripotent Stem Cell Derived from Human Fibroblasts[J].Cell Reprogram,2016,18(2):67-77.
[34] JIN H,CHENG X,PEI Y,et al.Identification and verification of transgelin-2 as a potential biomarker of tumor-derived lung-cancer endothelial cells by comparative proteomics[J].J Proteomics,2016,136:77-88.
[35] KONG X,WANG Y,LIU S,et al.CD105 Over-expression Is Associated with Higher WHO Grades for Gliomas[J].Mol Neurobiol,2016,53(5):3 503-3 512.
[36] TAWFIK A,AL-SHABRAWEY M,ROON P,et al.Alterations of retinal vasculature in cystathionine-Beta-synthase mutant mice,a model of hyperhomo-cysteinemia[J].Invest Ophthalmol Vis Sci,2013,54(2):939-949.
[37] NAVONE S E,MARFIA G,NAVA S,et al.Human and mouse brain-derived endothelial cells require high levels of growth factors medium for their isolation,in vitro maintenance and survival[J].Vascular cell,2013,5(1):10-18.
[38] MENDICHOVSZKY I A,CUTAJAR M,GORDON I.Reproducibility of the aortic input function (AIF) derived from dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) of the kidneys in a volunteer study[J].Eur J Radiol,2009,71(3):576-581.
[39] RATA M,COLLINS D J,DARCY J,et al.Assessment of repeatability and treatment response in early phase clinical trials using DCE-MRI:comparison of parametric analysis using MR-and CT-derived arterial input functions[J].Eur Radiol,2016,26(7):1 991-1 998.
[40] CARDENAS-RODRIGUEZ J,HOWISON C M,MATSUNAGA T O,et al.A reference agent model for DCE MRI can be used to quantify the relative vascular permeability of two MRI contrast agents[J].Magn Reson Imaging,2013,31(6):900-910.
[41] CUTAJAR M,MENDICHOVSZKY I A,TOFTS P S,et al.The importance of AIF ROI selection in DCE-MRI renography:reproducibility and variability of renal perfusion and filtration[J].Eur J Radiol,2010,74(3):e154-e160.
[42] MELBOURNE A,HIPWELL J,MODAT M,et al.The effect of motion correction on pharmacokinetic parameter estimation in dynamic-contrast-enhanced MRI[J].Phys Med Biol,2011,56(24):7 693-7 708.
[43] MERREM A D,ZOLLNER F G,REICH M,et al.A variational approach to image registration in dynamic contrast-enhanced MRI of the human kidney[J].Magn Reson Imaging,2013,31(5):771-777.
[44] ZOLLNER F G,SANCE R,ROGELJ P,et al.Assessment of 3D DCE-MRI of the kidneys using non-rigid image registration and segmentation of voxel time courses[J].Comput Med Imag Graphics,2009,33(3):171-781.
[45] KANG H Y,XIAO H L,CHEN J H,et al.Comparison of the Effect of Vessel Size Imaging and Cerebral Blood Volume Derived from Perfusion MR Imaging on Glioma Grading[J].AJNR Am J Neuroradiol,2016,37(1):51-57.
[46] HECTORS S J,JACOBS I,LOK J,et al.Improved Evaluation of Antivascular Cancer Therapy Using Constrained Tracer-Kinetic Modeling for Multiagent Dynamic Contrast-Enhanced MRI[J].Cancer Res,2018,78(6):1 561-1 570.
[47] GEORGIOU L,SHARMA N,BROADBENT D A.Estimating breast tumor blood flow during neoadjuvant chemotherapy using interleaved high temporal and high spatial resolution MRI[J].Magn Reson Med,2018,79(1):317-326.
[48] WILSON D J,DALL B J,GANGI A,et al.Imaging vascular and hemodynamic features of the brain using dynamic susceptibility contrast and dynamic contrast enhanced MRI[J].Neuroimage,2018,3.pii:S1053-8119(18)30389-6.
[49] ROBERTS H C,ROBERTS T P,LEY S,et al.Quanti-tative estimation of microvascular permeability in human brain tumors:correlation of dynamic Gd-DTPA-enhanced MR imaging with histopathologic grading[J].Acad Radiol,2002,9(Suppl 1):151-155.
[50] LEACH M O,MORGAN B,TOFTS P S,et al.Imaging vascular function for early stage clinical trials using dynamic contrast-enhanced magnetic resonance imaging[J].Eur Radiol,2012,22(7):1 451-1 464.
(收稿2017-01-17 修回2018-03-10)
本文引用信息:李运奇,尹先哲,汤韬,赵智伟.动态对比增强磁共振在脑胶质瘤病理级别中的诊断价值[J].中国实用神经疾病杂志,2018,21(13):1407-1412.DOI:10.12083/SYSJ.2018.13.332
Reference information:LI Yunqi,YIN Xianzhe,TANG Tao,ZHAO Zhiwei.The value of dynamic contrast enhanced MRI in the diagnosis of glioma pathology[J].Chinese Journal of Practical Nervous Diseases,2018,21(13):1407-1412.DOI:10.12083/SYSJ.2018.13.332