目的 探讨多PLD ASL在不同程度脑动脉硬化(CAS)血流灌注改变方面的临床应用。方法 前瞻性纳入2017-01—2018-05脑动脉硬化患者60例,均采用GE 3.0T超导磁共振行常规序列、脑血管成像(MRA)及三维动脉自旋标记成像(3D-pCASL)序列检查,依据3D-TOF MRA将患者分为脑动脉硬化轻、中、重度3组,分别测量3组不同脑叶脑血流量(CBF)值,并统计不同脑叶CBF值达峰时相。结果 3组不同PLD不同脑叶CBF值差异有统计学意义(P<0.05),随着脑动脉硬化程度加重,不同脑叶CBF
多PLD ASL在脑动脉硬化血流灌注中的临床应用
卢明聪1) 孟 云1) 徐行茹1) 周建国1)△ 马先军2)
南京中医药大学连云港附属医院 1)放射科 2)脑病科,江苏 连云港 222004
作者简介:卢明聪,Email:lygzyylmc@163.com
△通信作者:周建国,Email:13645132158@163.com
【摘要】 目的 探讨多PLD ASL在不同程度脑动脉硬化(CAS)血流灌注改变方面的临床应用。方法 前瞻性纳入2017-01—2018-05脑动脉硬化患者60例,均采用GE 3.0T超导磁共振行常规序列、脑血管成像(MRA)及三维动脉自旋标记成像(3D-pCASL)序列检查,依据3D-TOF MRA将患者分为脑动脉硬化轻、中、重度3组,分别测量3组不同脑叶脑血流量(CBF)值,并统计不同脑叶CBF值达峰时相。结果 3组不同PLD不同脑叶CBF值差异有统计学意义(P<0.05),随着脑动脉硬化程度加重,不同脑叶CBF值有下降趋势,且脑血流速度亦逐渐减慢,达峰时相发生延迟。结论 通过利用多PLD ASL量化不同脑叶CBF,同时观察其达峰时相,有助于脑动脉硬化脑血流量监测及缺血性脑血管病发病风险评估。
【关键词】 动脉自旋标记;脑动脉硬化;脑血流量;标记后延迟时间;缺血性脑血管病
【中图分类号】 R743 【文献标识码】 A 【文章编号】 1673-5110(2018)18-1986-05 DOI:10.12083/SYSJ.2018.18.440
Clinical application of multi-PLD ASL in cerebral arteriosclerosis blood perfusion analysis
LU Mingcong1),MENG Yun1),XU Xingru1),ZHOU Jianguo1),MA Xianjun2)
1)Department of Radiology,Lianyungang TCM Hospital Affiliated to Nanjing University of Chinese Medicine,Lianyungang 222004,China;2)Cerebrovascular Diseases,Lianyungang TCM Hospital Affiliated to Nanjing University of Chinese Medicine,Lianyungang 222004,China
【Abstract】 Objective To explore the clinical application of multiple PLD ASL in different degrees of cerebral arteriosclerosis (CAS) perfusion changes.Methods Prospective inclusion of 60 patients with cerebral arteriosclerosis from January 2017 to May 2018,all using GE3.0T superconducting magnetic resonance imaging routine,cerebrovascular imaging (MRA) and three-dimensional arterial spin label imaging (3D-pCASL) sequences.According to the 3D-TOF MRA,the patients were divided into three groups:mild,moderate and severe cerebral arteriosclerosis.The cerebral blood flow (CBF) values of the three groups were measured,and the CBF values of different brain lobe were counted.Results This study found that the CBF values of different brains in different groups of PLDs were different,which was statistically significant.As the degree of cerebral arteriosclerosis worsened,the CBF values of different brains decreased,and the cerebral blood flow velocity gradually decreased,the phase is delayed.Conclusion By using multiple PLD ASL to quantify CBF of different brain lobe and observing its peak phase,it is helpful to monitor cerebral blood flow cerebral arteriosclerosis and risk assessment of ischemic cerebrovascular disease.
【Key words】 Arterial spin labeling;Cerebral arteriosclerosis;Cerebral blood flow;Delayed time after labeling;Ischemic cerebrovascular disease
缺血性脑血管病主要由供血动脉狭窄或闭塞引起,脑动脉硬化(cerebral artery atherosclerosie,CAS)是脑血管病最重要也是最常见的原因[1-4]。CAS是一种慢性、进行性、多发性脑血管疾病,因供血动脉发生弥漫性粥样硬化、管壁增厚、管腔狭窄,甚至血管闭塞,导致脑组织血液循环障碍,引发缺血性脑血管病变[5-8]。由于绝大部分脑卒中患者的生理病理过程是无法逆转的,因此,对脑血管病的危险因素进行积极早期干预尤为重要[2,9-11]。本研究通过利用多PLD ASL量化不同脑叶CBF值,并观察其达峰时相,评估临床缺血性脑血管病发病风险。
1 资料与方法
1.1 一般资料 回顾性研究南京中医药大学连云港附属医院脑病科2017-01—2018-05收治脑动脉硬化患者60例,男34例,女26例,年龄45~80(60.5±7.8)岁。主要临床症状:头晕、头痛、肢体无力、偏瘫、失语等。入组标准:(1)3D-TOF MRA提示脑动脉硬化;(2)发病年龄40~80岁。排除标准:(1)颅内肿瘤、血管畸形者;(2)危重或昏迷患者;(3)既往大面积脑梗死或脑出血患者。本次研究经院伦理委员会批准,并取得患者家属的知情同意。
1.2 仪器与方法 采用美国GE Discovery 750 3.0T超导型磁共振扫描仪,头颅8通道相控线圈。常规序列包括T1WI、T2WI、T2FLAIR、DWI。3D-TOF MRA具体参数:TE 2.6 ms,TR 22 ms,反转角15°,视野220 mm×194 mm,矩阵256×224。3D-pC ASL具体扫描参数:TR/TE=5 369 ms/10.5 ms,FOV 24 cm×24 cm,分辨率512×8,NEX=3,标记后延迟时间(posted labeling delay,PLD):1 025 ms、2 025 ms、3 025 ms。
1.3 数据后处理与分析 将MRA原始图像经GE AW4.6工作站进行最大密度投影(maximum intensity projection,MIP),从不同角度观察脑血管改变,必要时对各动脉管径进行测量。颅内动脉硬化程度分级:(1)轻度:脑血管走行僵硬,管壁边缘稍毛糙,无明显狭窄管壁;(2)中度:脑血管纤细,走行僵直,管腔粗细不均匀;(3)重度:部分脑动脉闭塞、分支稀疏[3]。
3D-pCASL原始数据经GE AW4.6工作站Functool软件进行后处理,得到全脑脑血流量(cerebral blood flow,CBF)伪彩图,依据MRA对脑动脉硬化进行程度分级,同时测量3组不同PLD CBF伪彩图显示不同脑叶的CBF值,并观察不同脑叶的CBF达峰时相,测量过程中尽量避开脑室、脑沟及颅底等结构,图像分别由2名神经组影像诊断医师进行双盲法观察,当观察及测量结果出现偏差时,引入第3名诊断医师协商后判定最终结果。
1.4 统计学分析 采用SPSS 17.0软件包进行数据处理,计量资料以均数±标准差(x±s)表示,2组间比较采用独立样本t检验,P<0.05为差异有统计学意义。
2 结果
入组LA患者60例,其中1级17例,2级25例,3级18例。随着动脉硬化程度加重,3组不同脑叶的CBF值有下降趋势(P<0.05),且CBF达峰时相发生延迟。见表1~2。
表1 不同程度脑动脉硬化CBF值比较
Table 1 Comparison of CBF values in different degrees of cerebral arteriosclerosis
| 动脉硬化 |
n |
CBF平均值 |
| 轻度 |
17 |
55.87±3.16 |
| 中度 |
25 |
51.20±2.85 |
| 重度 |
18 |
42.69±2.59 |
| F值 |
|
150.428 |
| P值 |
|
<0.001 |
表2 不同程度脑动脉硬化PLD达峰时间比较
Table 2 Comparison of PLD peak time in different degrees of cerebral arteriosclerosis
| 动脉硬化 |
PLD达峰时间 |
合计 |
| 1 025 |
2 025 |
3 025 |
| 轻度 |
5 |
11 |
1 |
17 |
| 中度 |
6 |
14 |
5 |
25 |
| 重度 |
0 |
5 |
13 |
18 |
| 合计 |
12 |
30 |
18 |
60 |
| χ2值 |
|
|
|
32.296 |
| P值 |
|
|
|
<0.001 |
3 讨论
CAS由多种危险因素相互作用所致,临床研究证实其与脑血管疾病的发生率及病死率密切相关[4,12-15]。CAS以局灶性粥样硬化斑块为特征,伴随血管内膜损伤、脂质沉积及泡沫细胞增多,导致动脉管壁增厚、弹性降低、管腔狭窄,继而发生脑供血不足,甚至发生脑梗死[5,16-20]。
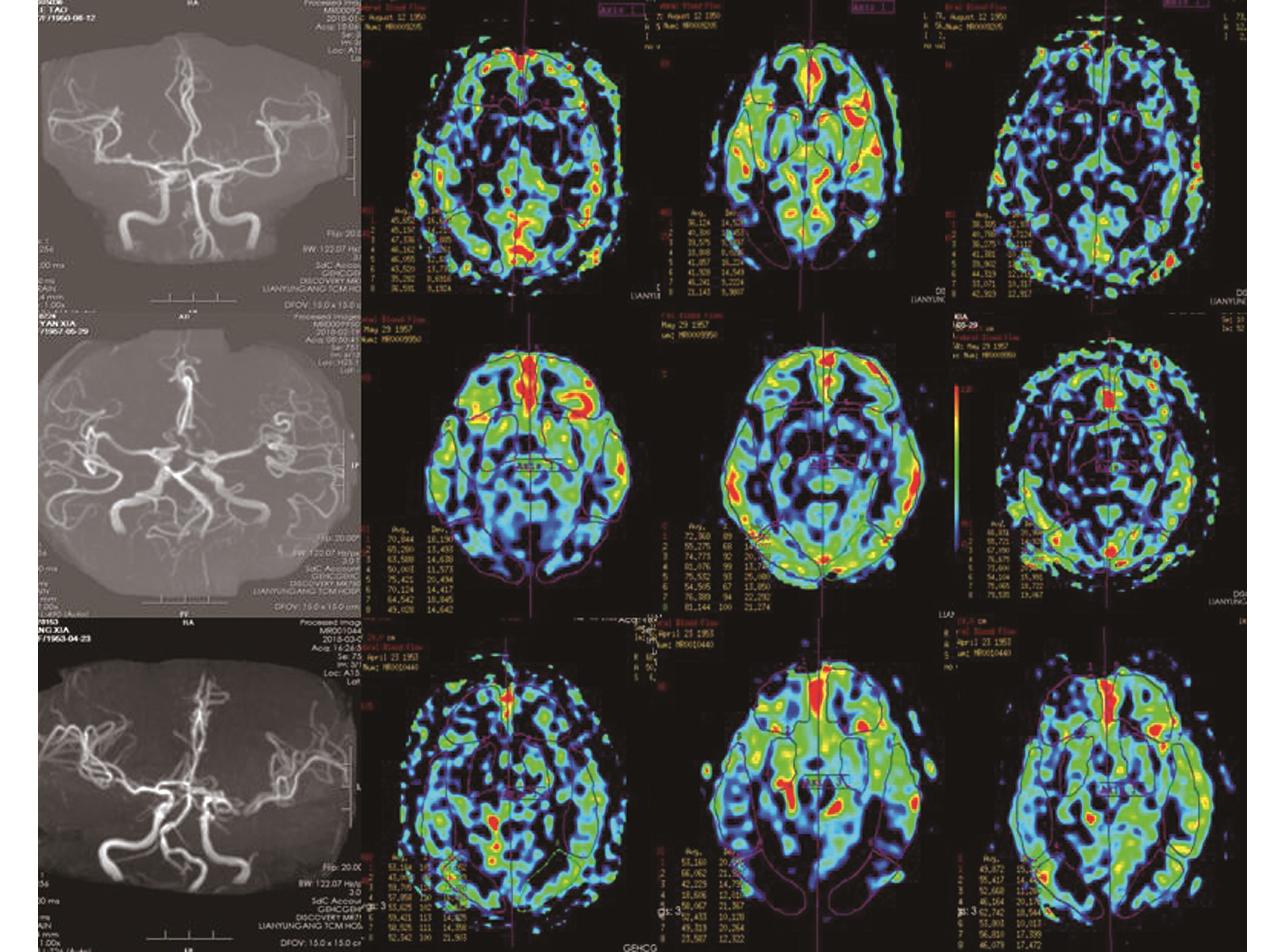
图1 A~D为同一病例,A:MRA提示轻度脑动脉硬化;B~D:ASL提示不同PLD脑叶CBF值,PLD达峰时间为2 025 ms;E~H为同一病例;E:MRA提示中度脑动脉硬化;F-H:ASL提示不同PLD脑叶CBF值,PLD达峰时间为2 025 ms;I~L为同一病例;I:MRA提示重度脑动脉硬化;J~L:ASL提示不同PLD脑叶CBF值,PLD达峰时间为3 025 ms
Figure 1 A~D is the same case,A:MRA suggests mild cerebral arteriosclerosis,B~D:ASL suggests CBF values in different PLD brain regions,PLD peak time is 2 025 ms;Figure E~H is the same case,E:MRA prompt Moderate cerebral arteriosclerosis,FH:ASL suggests CBF values in different PLD brain regions,PLD peak time is 2 025 ms;Figure I ~ L is the same case,I:MRA indicates severe cerebral arteriosclerosis;J ~ L:ASL tips are different PLD brain leaf CBF value,PLD peak time is 3 025 ms
磁共振血管造影(magnetic resonance angiography,MRA)因其具有安全无创、无需注射造影剂且可三维成像等优点,目前临床应用较为广泛[21-25]。因我国缺血性脑血管病患者颅内动脉狭窄率明显高于颅外动脉狭窄,对于动脉硬化高危人群均可进行MRA检查,评估脑动脉硬化程度[6,26-28]。但由于3D-TOF MRA对于容积内血流饱和效应较明显,在慢血流和容积内远端的血流显示较差[7,29-31]。
ASL通过将反转脉冲施加于颈部进行动脉血液标记,经过一定时间后,血液流入扫描层面,采集标记后血液信号,通过将标记相和未标记相进行剪影,即得到脑血流图,反映了某一时间流入局部脑组织的血流量[8,32-33]。3D-pCASL结合了CASL高信噪比与PASL高标记效能的优点,通过定量各脑区CBF值,能够较好评估脑灌注状况[9-10]。正常全脑CBF值50 mL/(100 g·min)左右,当CBF降低到10~20 mL/(100 g·min),或皮层的CBF降低到正常水平的40%,白质的CBF降低到正常水平的35%,才会出现脑组织缺血症状[11,34]。ASL可在无明显体征或症状轻微时即可准确评估脑血流量变化,由于CAS患者往往因动脉管壁或管腔病变导致血流动力学变化,使用单个PLD无法准确评估CBF。本研究通过利用多PLD(1 025 ms、2 025 ms、3 025 ms)ASL分析不同脑叶的CBF值,能够更加完整评估脑组织血流灌注量,较好避免单PLD评估脑灌注信息偏差,评判结果更为准确。本研究发现,3组不同PLD不同脑叶CBF值差异有明显统计学意义,随着脑动脉硬化程度加重,各组CBF值有下降趋势。目前在脑血管灌注信息监测方面,PWI应用较为成熟。PWI-TTP是DSC-PWI多参量图像总中反映缺血性脑血管病最敏感的指标,其主要反映缺血区血流达峰时间的延迟[12]。有定量研究亦显示,急性缺血性脑卒中患者ASL所显示的低灌注相对CBF值与PWI-MTT、TTP相对值具有较高的相关性,与PWI-TTP相关性最高[13]。本研究通过观察不同程度CAS脑叶CBF值达峰时相发现,随着动脉硬化程度的递增,脑血流速度亦逐渐减慢,达峰时间亦发生延迟,同时认为当重度动脉硬化存在血管闭塞时,部分存在侧支循环血流方面信息显示亦需要使用较长PLD才能够完整评估。
通过利用多PLD ASL量化脑实质CBF值及其达峰时相,有助于动脉硬化脑血流量监测,临床可进行缺血性脑血管病发病风险评估,进行早期预防及改善预后。但本文存在不足之处,仅针对颅内动脉硬化,未对颅外动脉硬化进行灌注研究,同时由于检查时间限制,未行更多PLD检测,统计结果可能会出现偏差,寄希望于以后的研究进一步深入。
4 参考文献
[1] 韩星伟.慢性缺血性脑血管病与脑动脉硬化性狭窄的关系[J].中国实用神经病疾病杂志,2017,20(11):130-131.
[2] 中华医学会神经病学分会,中华医学会神经病学分会脑血管病学组.中国脑血管病一级预防指南2015[J].中华神经科杂志,2015,48(8):629-643.
[3] 杨冠英,高明勇,张丽丽,等.脑动脉硬化、脑微出血与脑白质疏松分级的相关性研究[J].放射学实践,2017,31(7):679-682.
[4] NOVO S,PERITORE A,GUARNERI F P,et al.Metabolic syndrome(Mets) predicts cardioand cerebrovascu-lar events in a twenty years follow-up.A prospective study[J].Atherosclerosis,2012,223(2):468-472.
[5] 付文亭,李清,邵长娟,等.颅内动脉粥样硬化性狭窄与急性脑梗死进展发生的关系[J].中华老年心脑血管病杂志,2014,11(10):1 061-1 064.
[6] 周君,孙志宏,张钰,等.经颅多普勒和颈动脉超声检测高血压患者无症状性颅内外动脉粥样硬化病变[J].中风与神经疾病杂志,2014,31(4):345-347.
[7] 肖建明,陈志凡,陈云涛,等.提高3D TOF-MRA图像质量的研究[J].中国医疗设备,2013,28(10):158-161.
[8] 中华医学会放射学分会质量管理与安全管理学组,中华医学会放射学分会磁共振学组.动脉自旋标记脑灌注MRI技术规范化应用专家共识[J].中华放射学杂志,2016,50(11):817-824.
[9] 娄昕,吴冰,黄点点,等.正常成人后循环脑区动脉自选标记灌注成像的可重复性研究[J].中华放射学杂志,2014,48(2):151-154.
[10] 胡建斌,戴真煜,陈飞,等.磁共振三维动脉自旋标记成像不同标记延迟时间的比较及可重复性研究[J].医学影像学杂志,2017,27(3):402-406.
[11] 王利,郑罡,赵铁柱,等.动脉自旋标记技术在脑部疾病中的临床应用[J].生物医学工程学杂志,2013,30(1):195-199.
[12] 张水霞,张顺,姚义好,等.3D-ASL与DSC-PWI在缺血性脑梗死患者中的对比研究[J].放射学实践,2014,29(8):901-905.
[13] BIVARD A,STANWELL P,LEVI C,et al.Arterial spin labeling identifies tiggue salvage and good clinical recovery after acute ischemic stroke[J].J Neuroima-ging,2013,23(3):391-396.
[14] FUJIWARA Y,MATSUDA T,KANAMOTO M,et al.Comparison of long-labeled pseudo-continuous arterial spin labeling (ASL) features between young and elderly adults:special reference to parameter selection[J].Acta Radiol,2017,58(1):84-90.
[15] LIU T,CHENG G,KANG X,et al.Noninvasively evaluating the grading and IDH1 mutation status of diffuse gliomas by three-dimensional pseudo-continuous arterial spin labeling and diffusion-weighted imaging[J].Neuroradiology,2018,60(7):693-702.DOI:10.1007/s00234-018-2021-5.
[16] DAI Z Y,CHEN F,YAO L Z,et al.The combined application of magnetic resonance DTI and 3D-pcASL in differential diagnosis of hyper-acute and acute ischemic cerebral infarction[J].Zhonghua Yi Xue Za Zhi,2018,98(17):1 327-1 332.DOI:10.3760/cma.j.issn.0376-2491.2018.17.009.
[17] WANG Y L,CHEN S,XIAO H F,et al.Differentiation between radiation-induced brain injury and glioma recurrence using 3D pCASL and dynamic susceptibility contrast-enhanced perfusion-weighted imaging[J].Radiother Oncol,2018 Feb 1.pii:S0167-8140(18)30026-4.DOI:10.1016/j.radonc.2018.01.009.
[18] XU Q,LIU Q,GE H,et al.Tumor recurrence versus treatment effects in glioma:A comparative study of three dimensional pseudo-continuous arterial spin labeling and dynamic susceptibility contrast imaging[J].Medicine(Baltimore),2017,96(50):e9332.DOI:10.1097/MD.0000000000009332.
[19] YIN L,CHENG S,XIAO J,et al.3D pseudocontinuous arterial spin-labeling perfusion imaging detected crossed cerebellar diaschisis in acute,subacute and chronic intracerebral hemorrhage[J].Clin Imaging,2018,50:37-42.DOI:10.1016/j.clinimag.2017.12.007.
[20] WANG T,LI Y H,GUO X H,et al.Quantifying the Cerebral Hemodynamic Changes in Hypertensive Patients Using 3D Pseudo-continuous Arterial Spin Labeling[J].Zhongguo Yi Xue Ke Xue Yuan Xue Bao,2017,39(4):477-484.DOI:10.3881/j.issn.1000-503X.2017.04.004.
[21] DOLUI S,VIDORRETA M,WANG Z,et al.Compar-ison of PASL,PCASL,and background-suppressed 3D PCASL in mild cognitive impairment[J].Hum Brain Mapp,2017,38(10):5 260-5 273.DOI:10.1002/hbm.23732.
[22] JIA R,XU X,LIU X,et al.Value of 3D Pseudo-continuous Arterial Spin Labeling Magnetic Resonance Perfusion Imaging in Evaluating Posterior Circulation Ischemia in the Elderly[J].Zhongguo Yi Xue Ke Xue Yuan Xue Bao,2017,39(2):272-279.DOI:10.3881/j.issn.1000-503X.2017.02.018.
[23] AKSOY M,MACLAREN J,BAMMER R.Prospective motion correction for 3D pseudo-continuous arterial spin labeling using an external optical tracking system[J].Magn Reson Imaging,2017,39:44-52.DOI:10.1016/j.mri.2017.01.018.
[24] HAN P K,CHOI S H,PARK S H.Investigation of control scans in pseudo-continuous arterial spin labeling (pCASL):Strategies for improving sensitivity and reliability of pCASL[J].Magn Reson Med,2017,78(3):917-929.DOI:10.1002/mrm.26474.
[25] LIU W,LOU X,MA L.Use of 3D pseudo-continuous arterial spin labeling to characterize sex and age differences in cerebral blood flow[J].Neuroradiology,2016,58(9):943-948.DOI:10.1007/s00234-016-1713-y.
[26] LI R,XIAO H F,LYU J H,et al.Differential diagnosis of mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS) and ischemic stroke using 3D pseudocontinuous arterial spin labeling[J].J Magn Reson Imaging,2017,45(1):199-206.DOI:10.1002/jmri.25354.
[27] MAO C,FU Y,YE X,et al.Study of 3D-pcASL in differentiation of acute cerebral infarction and acute encephalitis[J].Zhonghua Yi Xue Za Zhi,2015,95(23):1 846-1 848.
[28] CHEN Y,DUAN M,ZHOU H L,et al.Three-dimensional Pseudo-continuous Arterial Spin Label Non-contrast Enhanced Perfusion Imaging of Head and Neck Tumors with High-field MR System[J].Zhongguo Yi Xue Ke Xue Yuan Xue Bao,2015,37(5):567-574.DOI:10.3881/j.issn.1000-503X.2015.05.013.
[29] WANG T,LI Y,GUO X,et al.Reduced perfusion in normal-appearing white matter in mild to moderate hypertension as revealed by 3D pseudocontinuous arterial spin labeling[J].J Magn Reson Imaging,2016,43(3):635-643.DOI:10.1002/jmri.25023.
[30] CHEN Z Y,GUAN Z W,YU S Y,et al.Comparison of 3D pseudo-continuous arterial spin labeling and positron emission tomography-computed tomography in the brain disorders[J].Zhongguo Yi Xue Ke Xue Yuan Xue Bao,2014,36(4):377-384.DOI:10.3881/j.issn.1000-503X.2014.04.006.
[31] HUANG D,WU B,SHI K,et al.Reliability of three-dimensional pseudo-continuous arterial spin labeling MR imaging for measuring visual cortex perfusion on two 3T scanners[J].PLoS One,2013,8(11):e79471.DOI:10.1371/journal.pone.0079471.
[32] ZUN Z,SHANKARANARAYANAN A,ZAHARCHUK G.Pseudocontinuous arterial spin labeling with prospective motion correction (PCASL-PROMO)[J].Magn Reson Med,2014,72(4):1 049-1 056.DOI:10.1002/mrm.25024.
[33] WONG A M,YAN F X,LIU H L.Comparison of three-dimensional pseudo-continuous arterial spin labeling perfusion imaging with gradient-echo and spin-echo dynamic susceptibility contrast MRI[J].J Magn Reson Imaging,2014,39(2):427-433.DOI:10.1002/jmri.24178.
[34] ROY B,AWASTHI R,BINDAL A,et al.Comparative evaluation of 3-dimensional pseudocontinuous arterial spin labeling with dynamic contrast-enhanced perfusion magnetic resonance imaging in grading of human glioma[J].J Comput Assist Tomogr,2013,37(3):321-326.DOI:10.1097/RCT.0b013e318282d7e2.
(收稿2018-06-15 修回2018-07-11)
本文引用信息:卢明聪,孟云,徐行茹,周建国,马先军.多PLD ASL在脑动脉硬化血流灌注中的临床应用[J].中国实用神经疾病杂志,2018,21(18):1986-1990.DOI:10.12083/SYSJ.2018.18.440
Reference information:LU Mingcong,MENG Yun,XU Xingru,ZHOU Jianguo,MA Xianjun.Clinical application of multi-PLD ASL in cerebral arteriosclerosis blood perfusion analysis[J].Chinese Journal of Practical Nervous Diseases,2018,21(18):1986-1990.DOI:10.12083/SYSJ.2018.18.440