目的 分析脑出血急性期血常规参数的变化与预后的关系。方法 将103例脑出血急性期患者纳入研究,30例健康检查者为正常组。脑出血急性期患者分组:按出血情况不同分为血肿扩大组、并发脑室出血组、出血量<30 mL组、出血量≥30 mL组,对比淋巴细胞计数、白细胞计数、中性粒细胞计数;按格拉斯哥昏迷指数(GCS)分为重度组、中度组和轻度组,对比急性期不同时间白细胞计数和中性粒细胞计数;按预后分为死亡、不良和良好组,对比白细胞计数和中性粒细胞计数。使用Logistic回归分析中性粒细胞、白细胞与脑出血急性期预后
脑出血急性期血常规参数的变化与预后的关系
吴 幸
平煤神马医疗集团,河南 平顶山 467099
基金项目:河南省医学科技攻关计划项目(201404H007)
作者简介:吴幸,Email:1912hanxiup@sina.com
【摘要】 目的 分析脑出血急性期血常规参数的变化与预后的关系。方法 将103例脑出血急性期患者纳入研究,30例健康检查者为正常组。脑出血急性期患者分组:按出血情况不同分为血肿扩大组、并发脑室出血组、出血量<30 mL组、出血量≥30 mL组,对比淋巴细胞计数、白细胞计数、中性粒细胞计数;按格拉斯哥昏迷指数(GCS)分为重度组、中度组和轻度组,对比急性期不同时间白细胞计数和中性粒细胞计数;按预后分为死亡、不良和良好组,对比白细胞计数和中性粒细胞计数。使用Logistic回归分析中性粒细胞、白细胞与脑出血急性期预后的关系及预测预后有效率。结果 出血量<30 mL组淋巴细胞与正常组差异无统计学意义(P>0.05),脑出血组白细胞、中性粒细胞计数与对照组比较差异有统计学意义(P<0.05);并发脑室出血患者中性粒细胞计数及白细胞计数均明显高于出血量<30 mL患者(P<0.05),但淋巴细胞计数差异无统计学意义(P>0.05)。入院时、入院后3 d、7 d,轻、中、重组白细胞计数及中性粒细胞计数差异有统计学意义(P<0.05),治疗15 d这种差异消失。死亡者白细胞计数及中性粒细胞计数最高(P<0.05)。脑积血患者白细胞计数上升77.14%,中性粒细胞上升71.43%。结论 脑出血急性期外周血白细胞计数和淋巴细胞计数不仅与病情严重程度有关,还与出血量、治疗时间相关,是评估预后的重要指标。
【关键词】 白细胞计数;中性粒细胞计数;脑出血急性期;淋巴细胞计数;预后
【中图分类号】 R743.34 【文献标识码】 A 【文章编号】 1673-5110(2018)19-2171-07 DOI:10.12083/SYSJ.2018.19.471
The relationship between the changes of blood routine parameters and the prognosis of patients with acute cerebral hemorrhage
WU Xing
Pingmei Shenma Medical Group Hospital,Pingdingshan 467099,China
【Abstract】 Objective To analyze the relationship between the change of blood routine parameters and the prognosis of patients with acute cerebral hemorrhage.Methods A total of 103 patients with acute cerebral hemorrhage were included in the study.Thirty healthy subjects were divided into normal group.Hemorrhage was divided into hematoma enlargement group,hemorrhage group <30 mL group,hemorrhage ≥30 mL group,contrast lymphocyte count,white blood cell count,neutrophil count;according to Glasgow Coma scale (GCS)were divided into severe group,moderate group and mild group.The white blood cell count and neutrophil count at different time of acute phase were compared.The patients were divided into death,bad and good groups according to the prognosis.The white blood cell count and neutrophil cell count.Logistic regression analysis of neutrophils,leukocytes and the prognosis of acute cerebral hemorrhage and prognosis of the relationship between the prognosis of effective.Results There was no significant difference between the group of blood loss <30 mL and the normal group(P>0.05).The leukocyte and neutrophil count of all cerebral hemorrhage groups were significantly different from those of the control group (P<0.05);the patients with intraventricular hemorrhage neutrophil count and white blood cell count were significantly higher than the bleeding <30 mL of patients(P<0.05),but no significant differences in lymphocyte count,P>0.05.There were significant differences in leukocyte count and neutrophil count between the two groups(P<0.05),and the difference disappeared at the 15th day of treatment.The death of white blood cell count and the highest neutrophil count(P<0.05).The increase rate of white blood cell count in patients with cerebral hemorrhage was 77.14%,neutrophils increased 71.43%.Conclusion The WBC count and lymphocyte count in peripheral blood are related not only with the severity of the disease,but also with the amount of bleeding and treatment time.It is an important index to evaluate the prognosis.
【Key words】 Leukocyte count;Neutrophil count;Acute cerebral hemorrhage;Lymphocyte;Prognosis
脑出血病因复杂,致死率高达41%,即使挽回生命,80%的患者有不同程度的残疾[1]。该病主要患病人群为老年人,在人口老龄化日益显著的情况下,成为我国人群第二大死因,且目前尚无有效治疗方法,治疗过程中耗费巨大物财力、人力,给家庭造成沉重负担,引起社会广泛关注。目前已知诱发因素包括工作压力、情绪波动、生活习惯、季节变换等,主要原因包括高血压合并动脉硬化、先天行脑动脉瘤、脑动脉炎、血管急性、血液病等,其中高血压合并动脉硬化是常见病因。
脑出血预后方面,目前国内外均有大量研究,炎症引起脑出血病理及生理改变逐渐被学者们认识,并发现降低白细胞计数、中性粒细胞数能缓解病情。国外研究发现,部分患者治疗几个月后其白细胞计数水平仍然较高,考虑与影响脑出血急性期患者白细胞计数的因素有关[2]。WANG等[3]研究发现,白细胞和中性粒细胞上升与脑出血急性期病死率有关。多种炎性因子阳性表达、炎性发展与其神经损伤联系密切,其中巨噬细胞、中性粒细胞浸润及其小胶质细胞为出血重要参与细胞,且巨噬细胞凋亡反应与神经元凋亡时间一致[4-5]。本研究探讨了中性粒细胞、淋巴细胞、白细胞计数与脑出血急性期患者预后的关系。
1 资料与方法
1.1 一般资料 收集脑出血急性期患者103例,男58例,女45例,年龄(66.2±6.2)岁;合并高血压75例,糖尿病47例;冠心病32例,有吸烟史42例,饮酒史53例。另选取30例来院健康检查的正常人群为正常组,男16例,女14例;年龄(65.3±4.9)岁;合并高血压24例,糖尿病13例,冠心病10例,有吸烟史12例,饮酒史14例。2组一般资料比较差异无统计学意义(P>0.05)。所有入选者均签署知情同意书。纳入标准:经头颅CT或MRI确诊,符合1995年全国第4次脑血管病学术会议关于脑血管疾病诊断标准;发病至入院时间≤24 h。排除标准:外伤、血液病、动脉炎所致脑出血,蛛网膜下腔出血,长期服用抗凝药,严重肝、肾疾病者。
1.2 方法
1.2.1 脑出血急性期患者分组:按出血情况不同分为血肿扩大组(图1)、并发脑室出血组(图2)、出血量<30 mL组(图3A)、出血量≥30 mL组(图3B);按格拉斯哥昏迷指数(GCS)分为重度组(3分≤GCS≤8分)、中度组(9分≤GCS≤12分)和轻度组(13分≤GCS≤14分)[6];按预后分为死亡组、不良(植物生存和中度、中度伤残)和良好组。
1.2.2 血常规检查:入院当天取外周静脉血,抗凝使用乙二胺四乙酸(EDTA)-K2,血常规检查使用全自动血细胞分析仪(日本SysmexXE-2100)。本研究分析的血常规参数包括中性粒细胞计数、白细胞计数和淋巴细胞计数。动态观察白细胞计数、淋巴细胞计数和中性粒细胞计数变化。分别于入院后3 d、7 d、15 d复查白细胞计数和中性粒细胞计数,考虑在对比不同出血情况中淋巴细胞计数未能明确区分正常组和出血量<30 mL组,且未能明确区分并发脑室出血组和出血量<30 mL组,因此,复查血常规时不再记录淋巴细胞计数动态变化。
1.3 统计学分析 使用SPSS 18.0 统计学软件分析数据,计量资料以均数±标准差(x±s)表示,行t检验,计数资料以率(%)表示,采用χ2检验。P<0.05为差异有统计学意义。使用Logistic回归分析中性粒细胞、白细胞与脑出血急性期预后的关系及预测预后有效率;中性粒细胞、白细胞进行Logistic回归分析,使用逐步入选法,当0.05<P<0.10则参考模型优势比结果;评估预测值时观察切割点(P)与中性粒细胞、白细胞预测脑抽出急性期不良预后和良好预后的关系,找到最佳切割点并记录良好预后和不良预后预测率。
2 结果
2.1 早期不同出血情况患者血常规指标对比 不同出现情况的脑出血组中性粒细胞及白细胞与对照组比较差异有统计学意义(P<0.05);出血量<30 mL组淋巴细胞与正常组差异无统计学意义(P>0.05),其余脑出血组与正常组淋巴细胞差异有统计学意义(P<0.05)。并发脑室出血患者中性粒细胞计数及白细胞计数均明显高于出血量<30 mL者(P<0.05),但淋巴细胞计数差异无统计学意义(P>0.05)。见表1。
2.2 急性期不同病情严重程度患者各时间段白细胞计数对比 入院时、入院后3 d、7 d,不同病情程度的三类患者白细胞计数及中性粒细胞计数组间比较差异有统计学意义(P<0.05)。随着治疗开展,3组白细胞计数和中性粒细胞计数均逐渐降低,入院后15 d 3组间比较差异无统计学意义(P>0.05)。见表2。
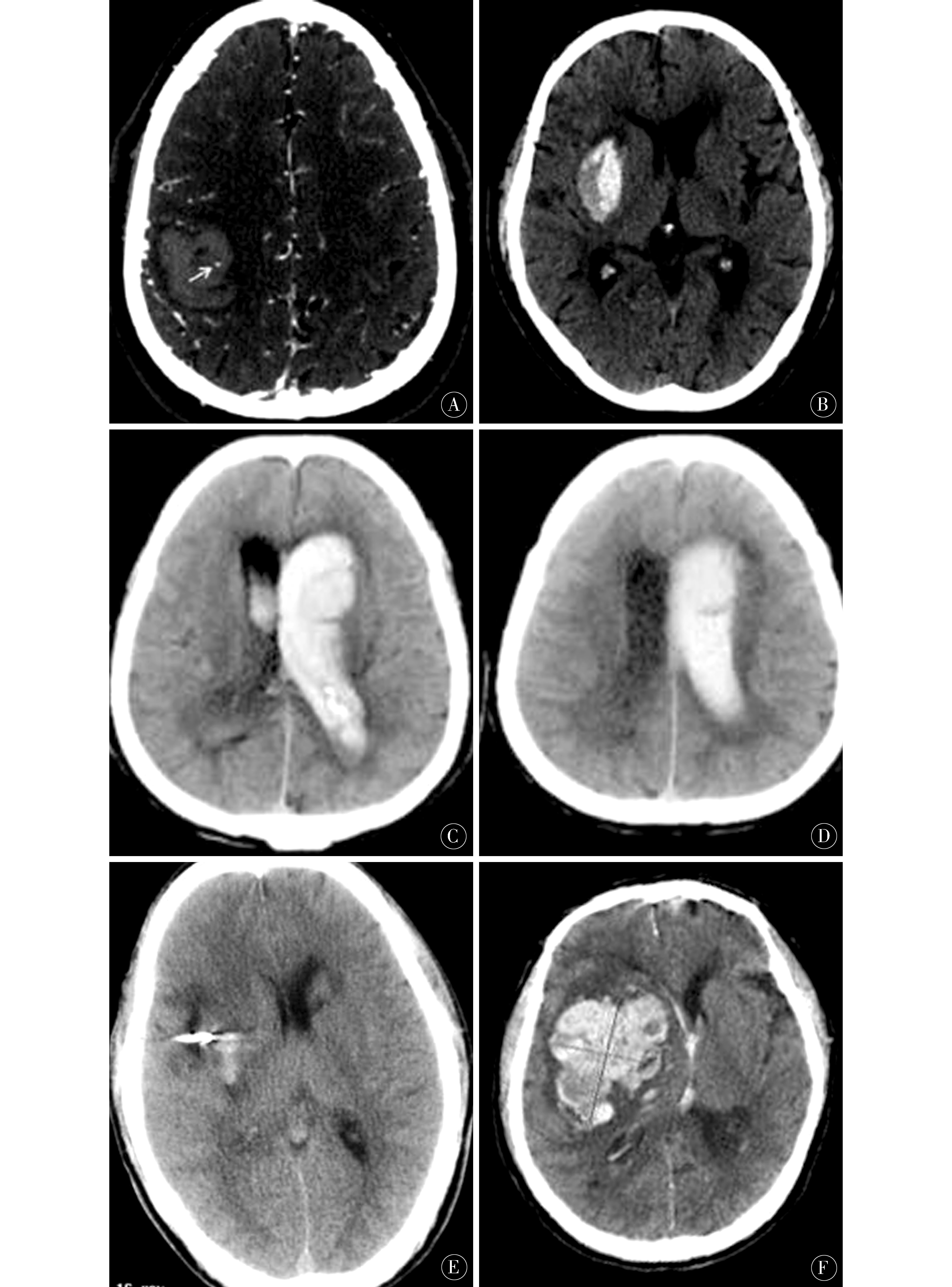
图1 A:箭头所指处有血肿扩大点状征,归血肿扩大组;B:血肿出现两种密度影,对位血肿扩大组;C、D:血肿破入脑室,归入并发脑室出血组;E:出血量<30 mL,约20 mL;F:出血量≥30 mL(约70 mL)
Figure 1 A:There is a hematoma enlargement point sign at the point of the arrow,and the hematoma enlargement group;B:Two density shadows appear in the hematoma, the contralateral hematoma enlargement group;C,D;hematoma broke into the ventricle,into the ventricular hemorrhage group;E:The amount of bleeding is <30 mL,about 20 mL;F:The amount of bleeding is ≥30 mL (about 70 mL)
2.3 出院时不同预后患者白细胞计数及中性粒细胞计数对比 死亡组中性粒细胞及白细胞最高,组间比较差异有统计学意义(P<0.05)。见表3。
2.4 预后判断模型分析结果 中性粒细胞和白细胞计数与预后相关,中性粒细胞为P=0.048,B=-0.215,白细胞计数为P=0.002,B=0.374。切割点为0.2时总体预测有效率较理想,预测预后不良有效率61.8%,预后良好有效率72.9%。
表1 急性期不同出血情况患者血常规指标对比 (x±s,×109个/L)
Table 1 Comparison of blood routine indicators in patients with different bleeding conditions in the acute phase (x±s,×109/L)
| 组别 |
n |
淋巴细胞 |
中性粒细胞 |
白细胞 |
| 正常组 |
30 |
2.33±0.84 |
5.11±1.79 |
7.06±1.78 |
| 血肿扩大组 |
20 |
1.28±0.67# |
7.74±3.10# |
9.06±3.46# |
| 并发脑室出血组 |
30 |
2.05±0.77# |
8.71±3.19#* |
10.62±4.12#* |
| 出血量≥30 mL组 |
18 |
1.72±0.81# |
8.09±3.49# |
9.49±3.65# |
| 出血量<30 mL组 |
35 |
2.11±0.72 |
6.19±2.46# |
8.29±2.61# |
| F值 |
|
6.58 |
7.89 |
5.37 |
| P值 |
|
0.0001 |
0 |
0.0005 |
注;与正常组比较,#P<0.05;与出血量<30 mL患者比较,*P<0.05
表2 急性期不同病情各时间段白细胞计数及中性粒细胞对比 (x±s,×109个/L)
Table 2 Comparison of white blood cell count and neutrophil comparison in different time periods in acute phase (x±s,×109/L)
| 指标 |
组别 |
n |
入院时 |
入院后3 d |
入院后7 d |
入院后15 d |
| 白细胞 |
重度 |
35 |
21.14±1.68 |
19.66±2.54 |
15.41±1.79 |
9.60±2.50 |
| |
中度 |
33 |
15.11±3.68 |
14.72±2.81 |
12.78±1.70 |
9.37±1.86 |
| |
轻度 |
35 |
12.67±4.70 |
11.57±2.61 |
10.05±2.37 |
9.00±1.49 |
| |
F值 |
|
51.76 |
82.9 |
46.11 |
0.8 |
| |
P值 |
|
0.000 0 |
0.000 0 |
0.000 0 |
0.452 4 |
| 中性粒细胞 |
重度 |
35 |
19.56±2.57 |
18.96±1.95 |
14.26±2.01 |
9.21±2.42 |
| |
中度 |
33 |
13.62±2.44 |
13.01±2.11 |
11.26±2.16 |
9.20±1.26 |
| |
轻度 |
35 |
11.36±3.95 |
10.62±2.56 |
8.52±2.01 |
8.95±1.65 |
| |
F值 |
|
66.24 |
130.24 |
74.54 |
0.22 |
| |
P值 |
|
0.000 0 |
0.000 0 |
0.000 0 |
0.803 0 |
表3 出院时不同预后患者白细胞计数及中性粒细胞计数对比 (x±s,×109个/L)
Table 3 Comparison of white blood cell count and neutrophil count in patients with different prognosis at discharge (x±s,×109/L)
| 预后 |
n |
中性粒细胞 |
白细胞 |
| 死亡 |
11 |
19.13±9.21 |
18.64±3.91 |
| 不良 |
30 |
17.74±1.53 |
16.27±0.69 |
| 良好 |
62 |
8.96±1.26 |
10.74±0.34 |
| F值 |
|
102.82 |
283.03 |
| P值 |
|
0.0000 |
0.0000 |
3 讨论
脑出血后患者外周血白细胞计数和中性粒细胞计数明显上升并高于健康者。本研究中无论是何种情况的出血,4组白细胞中性粒细胞计数和白细胞计数均明显高于正常组,主要原因:(1)以血肿形成压迫脑组织,增加颅内压,因此,丘脑-垂体轴内分泌改变,导致皮质醇激素和白细胞升高,患病后第1天会存在明显炎症反应,第2天炎症反应达到高峰,后期随之下降[7];(2)血肿压迫神经导致交感神经兴奋,白细胞计数增多;可溶细胞间黏附分子使白细胞黏附在血管壁,形成栓塞导致局部血液循环不足,脑组织缺氧缺血[8-9];(3)白细胞分泌的缩血管物质加剧血管收缩,使缺血情况更严重,白细胞活化后使血脑屏障通透性增加,损伤脑实质[10-11];(4)白细胞浸润激活小胶质细胞,并释放血小板活化因子、蛋白水解酶、氧自由基等,破坏血管内皮细胞,增加血管壁通透性,加剧水肿,降低颅内灌注,加重脑缺氧缺血[12-13]。中性粒细胞与脑出血病情有关的机制可能是[14-15]:嗜中性粒细胞产生的超痒阴离子等自由基不断增加,导致脑组织脂质过氧化,基质金属蛋白酶被激活,血脑屏障透性增高,遭到破坏,且嗜中性粒细胞产生的自由基可诱导脑组织细胞凋亡,因此,使脑组织损伤加重[16-17]。
并发脑室出血是脑出血预后独立危险因素。本研究中并发脑室出血的患者中性粒细胞计数及白细胞计数均明显高于出血量<30 mL者(P<0.05)。入院时、入院后3 d、7 d,不同病情程度的三类患者白细胞计数及中性粒细胞计数比较差异有统计学意义(P<0.05),提示白细胞计数和中性粒细胞计数与脑出血急性期病情严重程度和出血情况有关。这可能与白细胞计数和中性粒细胞计数升高可加重脑组织缺血缺氧,加重水肿等有关[18-19]。此外,本研究发现,治疗15 d时轻度、中度、重度患者对比中性粒细胞计数和白细胞计数均无明显差异。研究发现,脑出血早期患者中性粒细胞和白细胞计数均上升,3 d时均明显降低,3周时逐渐倾向正常,与本研究一致。但国内也有研究认为,观察白细胞计数可延长观察时间到脑出血后3个月[20]。
直接从出院时患者预后来看,死亡患者白细胞计数和中性粒细胞计数均仍保持在高水平,与不良与后和良好预后均存在显著差异。研究发现,当脑出血急性期患者白细胞计数≥15×109个/L时病死率明显增加,治疗无效率也明显增加[21-22],与本研究一致。考虑因白细胞升高后血浆肌酸激酶被激活并快速升高,从而使胞质血管壁结构被破坏,引起微循环障碍;白细胞浸润生成的活性物对脑血管和脑神经细胞有直接破坏作用[23-35]。本研究通过回归分析发现,白细胞计数、中性粒细胞计数与脑出血急性期预后密切相关,其能辅助脑出血急性期预后预测,指导临床治疗。相关研究表明,小鼠脑出血后炎性细胞会有一定程度升高,损伤程度与神经功能损伤程度联系密切[36-48]。积极予以有效措施干预炎性反应,能积极控制脑出血后组织损伤,对疾病预后有重要临床意义。
4 参考文献
[1] CHAN E,ANDERSON C S,WANG X,et al.Signifi-cance of Intraventricular Hemorrhage in Acute Intracerebral Hemorrhage Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial Results[J].Stroke,2015,46(3):653-658.
[2] LATTANZI S,BRIGO F,TRINKA E,et al.Neutrophil-to-Lymphocyte Ratio in Acute Cerebral Hemorrhage:a System Review[J].Transl Stroke Res,2018 Aug 8.doi:10.1007/s12975-018-0649-4.
[3] WANG X,ARIMA H,YANG J,et al.Mannitol and Outcome in Intracerebral Hemorrhage Propensity Score and Multivariable Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial 2 Results[J].Stroke,2015,46(10):2 762-2 767.
[4] 卢艳秋,刘小军,常克亮,等.不同时间炎性因子白细胞介素-1β、肿瘤坏死因子-α表达与脑出血患者神经细胞凋亡的关系[J].中华实验外科杂志,2016,33(12):2 780-2 782.
[5] LATTANZI S,CAGNETTI C,PROVINCIALI L,et al.Neutrophil-to-lymphocyte ratio and neurological deterioration following acute cerebral hemorrhage[J].Oncotarget,2017,8(34):57 489-57 494.doi:10.18632/oncotarget.15423.
[6] TAO C,WANG J,HU X,et al.Clinical Value of Neutrophil to Lymphocyte and Platelet to Lymphocyte Ratio After Aneurysmal Subarachnoid Hemorrhage[J].Neurocrit Care,2017,26(3):393-401.doi:10.1007/s12028-016-0332-0.
[7] SUN Y,YOU S,ZHONG C,et al.Neutrophil to lymphocyte ratio and the hematoma volume and stroke severity in acute intracerebral hemorrhage patients[J].Am J Emerg Med,2017,35(3):429-433.doi:10.1016/j.ajem.2016.11.037.
[8] 田丽芹,张云书,薛新琴,等.基底节区脑出血患者发生早期神经功能恶化的危险因素分析[J].疑难病杂志,2015,17(8):789-792.
[9] 杨永凯,张帆,薛少华,等.血清和肽素、降钙素原对脑出血合并肺部感染早期诊断及判断预后的价值[J].重庆医学,2015,(18):2 483-2 484;2 487.
[10] 何磊磊,孙正杰,郭艳霞,等.血清胶质纤维酸性蛋白C反应蛋白及和肽素联合MICH评分在自发性脑出血患者预后判断中的价值[J].中国急救医学,2016,36(6):502-506.
[11] LATTANZI S,SILVESTRINI M.Response by Lattanzi and Silvestrini to Letter Regarding Article,”Neutrop-hil-to-Lymphocyte Ratio Predicts the Outcome of Acute Intracerebral Hemorrhage”[J].Stroke,2016,47(8):e217.doi:10.1161/STROKEAHA.116.014263.
[12] 孟晓峰,史保中,乔鹏,等.血清hs-CRP、TNF-α在脑出血昏迷患者中的动态变化及临床意义[J].中国实验诊断学,2017,21(6):945-947.
[13] 饶春光,王宏.脑出血患者相关炎症因子变化与预后的相关性研究[J].河北医学,2015,23(7):1 088-1 092.
[14] 李新玲,黄怀宇,朱易华,等.中性粒细胞碱性磷酸酶在急性脑出血患者并发感染中的诊断价值[J].中华临床感染病杂志,2016,9(6):513-517;532.
[15] DU R,LI D,ZHANG Q.Letter by Du et al Regarding Article,”Neutrophil-to-Lymphocyte Ratio Predicts the Outcome of Acute Intracerebral Hemorrhage”[J].Stroke,2016,47(8):e216.doi:10.1161/STROKEAHA.116.014216.
[16] 陶冶,薛维爽,滕伟禹,等.脑出血患者外周血中性粒细胞/淋巴细胞和血小板/淋巴细胞比值的临床意义[J].中国现代医学杂志,2017,27(8):80-84.
[17] 陆丙丁,王川.脉血康肠溶片在治疗急性脑出血患者水肿、促进脑血肿吸收中的作用[J].海南医学院学报,2016,22(19):2 287-2 289.
[18] IKEDA T,AMIZUKA T,ITO Y,et al.Changes in the perfusion waveform of the internal cerebral vein and intraventricular hemorrhage in the acute management of extremely low-birth-weight infants[J].Eur J Pediatr,2015,174(3):331-338.
[19] LATTANZI S,CAGNETTI C,PROVINCIALI L,et al.Neutrophil-to-Lymphocyte Ratio Predicts the Outcome of Acute Intracerebral Hemorrhage[J].Stroke,2016,47(6):1 654-1 657.doi:10.1161/STROKEAHA.116.013627.
[20] 邢浩,黄录茂,袁荣强,等.高血压脑出血术后外周血单核细胞计数与近期预后关系[J].安徽医学,2016,37(5):543-546.
[21] 宇宏,张志珺.外周血中性粒细胞/淋巴细胞值与脑血管病相关性研究进展[J].东南大学学报(医学版),2017,36(2):275-279.
[22] 封萍,廖谷清,贺承健,等.中性粒细胞与淋巴细胞比值对脑卒中相关性肺炎的预测价值[J].中国现代医学杂志,2017,27(15):97-102.
[23] 徐玢,张初吉,李建国,等.高渗盐水对重症脑出血的免疫调节作用研究[J].中国医药导报,2015,27(11):88-92.
[24] WANG F,HU S,DING Y,et al.Neutrophil-to-Lymphocyte Ratio and 30-Day Mortality in Patients with Acute Intracerebral Hemorrhage[J].J Stroke Cerebrovasc Dis,2016,25(1):182-187.doi:10.1016/j.jstrokecerebrovasdis.2015.09.013.
[25] 吴婵姬,黄仕雄.脑出血与脑梗死患者D-二聚体和凝血功能指标的变化研究[J].中国实用神经疾病杂志,2018,21(4):399-401.
[26] ARAI N,MINE Y,KAGAMI H,et al.The Diffuse and Severe Traumatic Subarachnoid Hemorrhage Being Hard to Distinguish to Aneurysmal Subarachnoid Hemorrhage[J].J Craniofac Surg,2018 Nov 15.doi:10.1097/SCS.0000000000004908.
[27] CONZEN C,BECKER K,ALBANNA W,et al.The Acute Phase of Experimental Subarachnoid Hemorrha-ge:Intracranial Pressure Dynamics and Their Effect on Cerebral Blood Flow and Autoregulation[J].Transl Stroke Res,2018 Nov 15.doi:10.1007/s12975-018-0674-3.
[28] INOUE T,ISHIDA T,INOUE T,et al.Lectin-Like Oxidized Low-Density Lipoprotein Receptor-1 Levels as a Biomarker of Acute Intracerebral Hemorrhage[J].J Stroke Cerebrovasc Dis,2018 Nov 12.doi:10.1016/j.jstrokecerebrovasdis.2018.10.027.
[29] TOYODA K,KOGA M,YAMAMOTO H,et al.Clinical outcomes depending on acute blood pressure after cerebral hemorrhage[J].Ann Neurol,2018 Nov 12.doi:10.1002/ana.25379.
[30] MOULLAALI T J,WANG X,MARTIN R H,et al.Statistical analysis plan for pooled individual patient data from two landmark randomized trials (INTERACT2 and ATACH-II) of intensive blood pressure lowering treatment in acute intracerebral hemorrhage[J].Int J Stroke,2018 Nov 12:1747493018813695.doi:10.1177/1747493018813695.
[31] AMULURU K,AL-MUFTI F,ROMERO C E,et al.Isolated Intraventricular Hemorrhage Associated with Cerebral Vasospasm and Delayed Cerebral Ischemia following Arteriovenous Malformation Rupture[J].Interv Neurol,2018,7(6):479-489.doi:10.1159/000490583.
[32] LIU K,PEI L,GAO Y,et al.Dehydration Status Predicts Short-Term and Long-Term Outcomes in Patients with Cerebral Venous Thrombosis[J].Neurocrit Care,2018 Oct 25.doi:10.1007/s12028-018-0628-3.
[33] KHALAYLEH H,LIN G,KADAR SFARAD H,et al.Traumatic Minor Intracranial Hemorrhage:Management by Non-neurosurgeon Consultants in a Regional Trauma Center is Safe and Effective[J].World J Surg,2018 Oct 25.doi:10.1007/s00268-018-4821-5.
[34] LAW Z K,SALMAN R A,BATH P M,et al.Hemostatic Therapies For Acute Spontaneous Intracerebral Hemorrhage[J].Stroke,2018,49(8):e271-e272.doi:10.1161/STROKEAHA.118.022071.
[35] ISMAIL M,ARMOIRY X,TAU N,ZHU F,et al.Mothership versus drip and ship for thrombectomy in patients who had an acute stroke:a systematic review and meta-analysis[J].J Neurointerv Surg,2018 Oct 8.doi:10.1136/neurintsurg-2018-014249.
[36] JIANG B,BENDER M T,WESTBROEK E M,et al.Procedural complexity independent of P2Y12 reaction unit (PRU) values is associated with acute in situ thrombosis in Pipeline flow diversion of cerebral aneurysms[J].Stroke Vasc Neurol,2018,3(3):169-175.doi:10.1136/svn-2018-000150.
[37] UNGVARI Z,YABLUCHANSKIY A,TARANTINI S,et al.Repeated Valsalva maneuvers promote symptomatic manifestations of cerebral microhemorrhages:implications for the pathogenesis of vascular cognitive impairment in older adults[J].Geroscience,2018 Oct 4.doi:10.1007/s11357-018-0044-9.
[38] CHOI P K,CHUNG J Y,LEE S J,et al.Recurrent cerebral microbleeds with acute stroke symptoms:A case report[J].Medicine (Baltimore),2018,97(39):e12480.doi:10.1097/MD.0000000000012480.
[39] HOWE M D,ZHU L,SANSING L H,et al.Serum Markers of Blood-Brain Barrier Remodeling and Fibrosis as Predictors of Etiology and Clinicoradiologic Outcome in Intracerebral Hemorrhage[J].Front Neurol,2018,9:746.doi:10.3389/fneur.2018.00746.
[40] KAZMI S O,ACHI O,DAMANI R.Full-Dose Thrombolysis for a Right Middle Cerebral Artery Stroke after an Acute Aortic Dissection[J].Ann Indian Acad Neurol,2018,21(3):223-224.doi:10.4103/aian.AIAN_78_18.
[41] DI NAPOLI M,SLEVIN M,POPA-WAGNER A,et al.Monomeric C-Reactive Protein and Cerebral Hemorrhage:From Bench to Bedside[J].Front Immunol,2018,9:1 921.doi:10.3389/fimmu.2018.01921.
[42] BOLTZE J,FERRARA F,HAINSWORTH A H,et al.Lesional and perilesional tissue characterization by automated image processing in a novel gyrencephalic animal model of peracute intracerebral hemorrhage[J].J Cereb Blood Flow Metab,2018 Sep 21:271678X18802119.doi:10.1177/0271678X18802119.
[43] DE BOYSSON H,PARIENTI J J,MAWET J,et al.Primary angiitis of the CNS and reversible cerebral vasoconstriction syndrome:A comparative study[J].Neurology,2018,91(16):e1468-e1478.doi:10.1212/WNL.0000000000006367.
[44] ZHANG Q,ZENG L,CHEN X,et al.Clinical Evalua-tion of Herbal Medicine (ICH-012) in Treating Acute Cerebral Haemorrhage:Safety and Efficacy from 6-to 72-Hour Time Window (CRRICHTrial-II)[J].Evid Based Complement Alternat Med,2018,2 018:3120179.doi:10.1155/2018/3120179.
[45] LIU Z,CHAI E,CHEN H,et al.Comparison of Thrombelastography (TEG) in Patients with Acute Cerebral Hemorrhage and Cerebral Infarction[J].Med Sci Monit,2018,24:6 466-6 471.doi:10.12659/MSM.910121.
[46] YAMAGUCHI Y,KOGA M,SATO S,et al.Early Achievement of Blood Pressure Lowering and Hematoma Growth in Acute Intracerebral Hemorrhage:Stroke Acute Management with Urgent Risk-Factor Assessment and Improvement-Intracerebral Hemorrhage Study[J].Cerebrovasc Dis,2018,46(3/4):116-122.doi:10.1159/000492728.
[47] GERNER S T,AUERBECK K,SPRGEL M I,et al.Peak Troponin I Levels Are Associated with Functional Outcome in Intracerebral Hemorrhage[J].Cerebrovasc Dis,2018,46(1/2):72-81.doi:10.1159/000492395.
[48] LANDRENEAU M J,MULLEN M T,MESS S R,et al.CCL2 and CXCL10 are associated with poor outcome after intracerebral hemorrhage[J].Ann Clin Transl Neurol,2018,5(8):962-970.doi:10.1002/acn3.595.
(收稿2016-12-20 修回 2018-08-10)
本文责编:夏保军
本文引用信息:吴幸.脑出血急性期血常规参数的变化与预后的关系[J].中国实用神经疾病杂志,2018,21(19):2171-2177.DOI:10.12083/SYSJ.2018.19.471
Reference information:WU Xing.The relationship between the changes of blood routine parameters and the prognosis of patients with acute cerebral hemorrhage[J].Chinese Journal of Practical Nervous Diseases,2018,21(19):2171-2177.DOI:10.12083/SYSJ.2018.19.471