目的 探讨正常人视神经的形态及特征,对比三维超声和多层螺旋CT扫描重建方法测量的正常人眶内段视神经的参数。方法 2015-06—2017-12在河南省人民医院放射科行颅脑CT检查的24~65岁的成年人102人102眼,采用多层螺旋CT扫描后对眶内段视神经重建,并对上述102眼做三维超声眶内段视神经成像,在超声图像和CT图像上分别测量距球后视神经起始部3、6、9、12 mm处视神经横断面最长径、最短径及面积,分析随着距视神经起始部距离的延长上述视神经参数的变化,并分析两种成像方式下测量的上述视神经参数是否有
三维超声与多层螺旋CT扫描重建在正常人眶内段视神经的参数测量及对比研究
刘银龙 吴 刚 孔 莎 罗帅伟 朱丽敏△
河南省人民医院(郑州大学人民医院)超声科,河南 郑州 450003
基金项目:国家卫生计生委2013-2014国家临床重点专科建设项目(2013226)
作者简介:刘银龙,Email:514378385@qq.com
△通信作者:朱丽敏,Email:1050054285@qq.com
【摘要】 目的 探讨正常人视神经的形态及特征,对比三维超声和多层螺旋CT扫描重建方法测量的正常人眶内段视神经的参数。方法 2015-06—2017-12在河南省人民医院放射科行颅脑CT检查的24~65岁的成年人102人102眼,采用多层螺旋CT扫描后对眶内段视神经重建,并对上述102眼做三维超声眶内段视神经成像,在超声图像和CT图像上分别测量距球后视神经起始部3、6、9、12 mm处视神经横断面最长径、最短径及面积,分析随着距视神经起始部距离的延长上述视神经参数的变化,并分析两种成像方式下测量的上述视神经参数是否有差异。结果 CT扫描重建后获得的各位点间视神经横断面的最长径、最短径及面积的总体比较差异均有统计学意义(F=214.218、213.814、239.987,均P=0.001)。三维超声成像获得的上述参数较差异也有统计学意义(F=237.325、219.763、250.362,均P=0.001)。CT扫描重建与三维超声成像两种方式均发现随着距球后视神经起始部的增大,视神经逐渐变细。CT扫描重建与三维超声成像获得的距球后视神经起始部3、6、9、12 mm处视神经横断面最长径分别为(6.13±0.39)/(6.38±0.32)、(5.35±0.45)/(5.65±0.37)、(5.10±0.39)/(5.01±0.31)、(4.78±0.43)/(4.65±0.27)mm;最短径分别为(5.52±0.47)/(5.65±0.37)、(4.89±0.43)/(4.95±0.29)、(4.59±0.34)/(4.47±0.31)、(4.36士0.29)/(4.35±0.37)mm;面积分别为(27.28±3.82)/(27.49±4.12)、(22.13±3.24)/(23.08±3.73)、(19.24±2.81)/(18.54±2.65)、(17.13±2.67)/(17.43±3.07)mm2,上述两种方式获得的参数比较差异均无统计学意义(P>0.05)。结论 三维超声与多层螺旋CT扫描后重建均可用于研究眶内段视神经,可为诊断眶内段视神经病变提供帮助。
【关键词】 眶内段视神经病变;视神经;三维超声;CT重建;正常人
【中图分类号】 R774.6 【文献标识码】 A 【文章编号】 1673-5110(2018)18-1978-08 DOI:10.12083/SYSJ.2018.18.439
Parametric measurement and comparative study of three-dimensional ultrasound and multi-slice spiral CT reconstruction in the optic nerve of normal human sacral
LIU Yinlong,WU Gang,KONG Sha,LUO Shuaiwei,ZHU Limin
Department of Ultrasound,People's Hospita of Henan Province(People's Hospital of Zhengzhou University),Zhengzhou 450003,China
【Abstract】 Objective To explore the morphology and characteristics of the normal human optic nerve,and compare the parameters of the optic nerve in the normal human sacral sac measured by three-dimensional ultrasound and multi-slice spiral CT scan reconstruction.Methods From June 2015 to December 2017,102 eyes of 102 adults aged 24-65 years old adults in the Department of Radiology,People's Hospital of Henan Province,were treated with multi slice spiral CT scan to reconstruct the optic nerve in the orbital segment,and the above 102 eyes were treated with three-dimensional ultrasonic optic nerve imaging.The initial optic nerve was measured on the ultrasonic image and the CT image.The longest diameter,the shortest diameter and area of the optic nerve in the 3,6,9,12 mm sections were observed,and the changes of the above optic nerve parameters were analyzed with the distance from the beginning of the optic nerve,and there was no statistical difference between the parameters of the optic nerve measured under the two imaging methods.Results The overall difference of the longest diameter,the shortest diameter and area of the optic nerve cross section after CT scanning was statistically significant (F=214.218,213.814,239.987,P=0.001).The above parameters obtained by three dimensional ultrasound imaging were also statistically significant (F=237.325,219.763,250.362,P=0.001).The two methods of CT scan reconstruction and three-dimensional ultrasound imaging showed that the optic nerve gradually became thinner with the increase of the optic nerve origin.The longest diameter of the optic nerve transverse section at 3,6,9,12 mm of the posterior optic nerve after CT scanning was respectively (6.13±0.39),(5.35±0.45),(5.10±0.39) and (4.78±0.43) mm.The longest transverse section of optic nerve at 3,6,9,12 mm of the posterior optic nerve obtained by three-dimensional ultrasound imaging was (6.38±0.32),(5.65±0.37),(5.01±0.31),(4.65±0.27)mm respectively;The shortest transverse section of optic nerve was (5.52±0.47)/(5.65±0.37),(4.89±0.43)/(4.95±0.29),(4.59±0.34)/(4.47±0.31),(4.36士0.29)/(4.35±0.37)mm.The area was(27.28±3.82)/(27.49±4.12),(22.13±3.24)/(23.08±3.73),(19.24±2.81)/(18.54±2.65),(17.13±2.67)/(17.43±3.07)mm2.There was no significant difference in the parameters obtained in the two ways (P>0.05).Conclusion Both three-dimensional ultrasound and multi-slice spiral CT reconstruction can be used to study the optic nerve in the iliac crest,which can help to diagnose the optic neuropathy in the iliac crest.
【Key words】 Intraorbital optic neuropathy;Optic nerve;Three-dimensional ultrasound;CT reconstruction;Normal human
许多疾病可引起视神经的形态学改变,通过观察视神经形态学有无改变可以推断是否存在疾病[1-5]。以往观察球后视神经通常依赖二维超声、普通CT或MRI等设备[6-8],通常获得的图像不够清晰直观[9]。随着三维超声的广泛应用,浅表器官的三维超声扫描技术也逐渐开始应用于临床。随着CT设备及软件的不断升级更新,多层螺旋CT扫描后重建在眶内段视神经的检测方面也得到应用[10]。本文就多层螺旋CT扫描后重建在眶内段视神经的探测进行研究,并对比分析三维超声成像及多层螺旋CT扫描后重建两种方式获得的眶内段视神经的参数,为诊断视神经疾病或视神经相关颅内疾病提供依据。
1 资料与方法
1.1 一般资料 2015-06—2017-12在河南省人民医院放射科行颅脑CT检查并自愿接受三维超声眼部检查的自愿者102人102眼,均为24~65岁的成年人,其中女53例,男49例;年龄24~65(45.35±19.33)岁。选择健康侧眼,其中左眼46眼,右眼56眼。纳入标准:(1)CT扫描健康侧眼视觉传导通路未见异常者;(2)健侧裸眼视力或最佳矫正视力≥1.0者。排除标准:(1)有神经系统疾病或手术史者;(2)有眼科或全身疾病者可引起视神经改变的。受检者分别由专门超声医师和放射科医师行三维超声及CT检查。本研究设计遵守赫尔辛基宣言并经河南省人民医院临床研究伦理委员会同意,受检者均签署知情同意书。
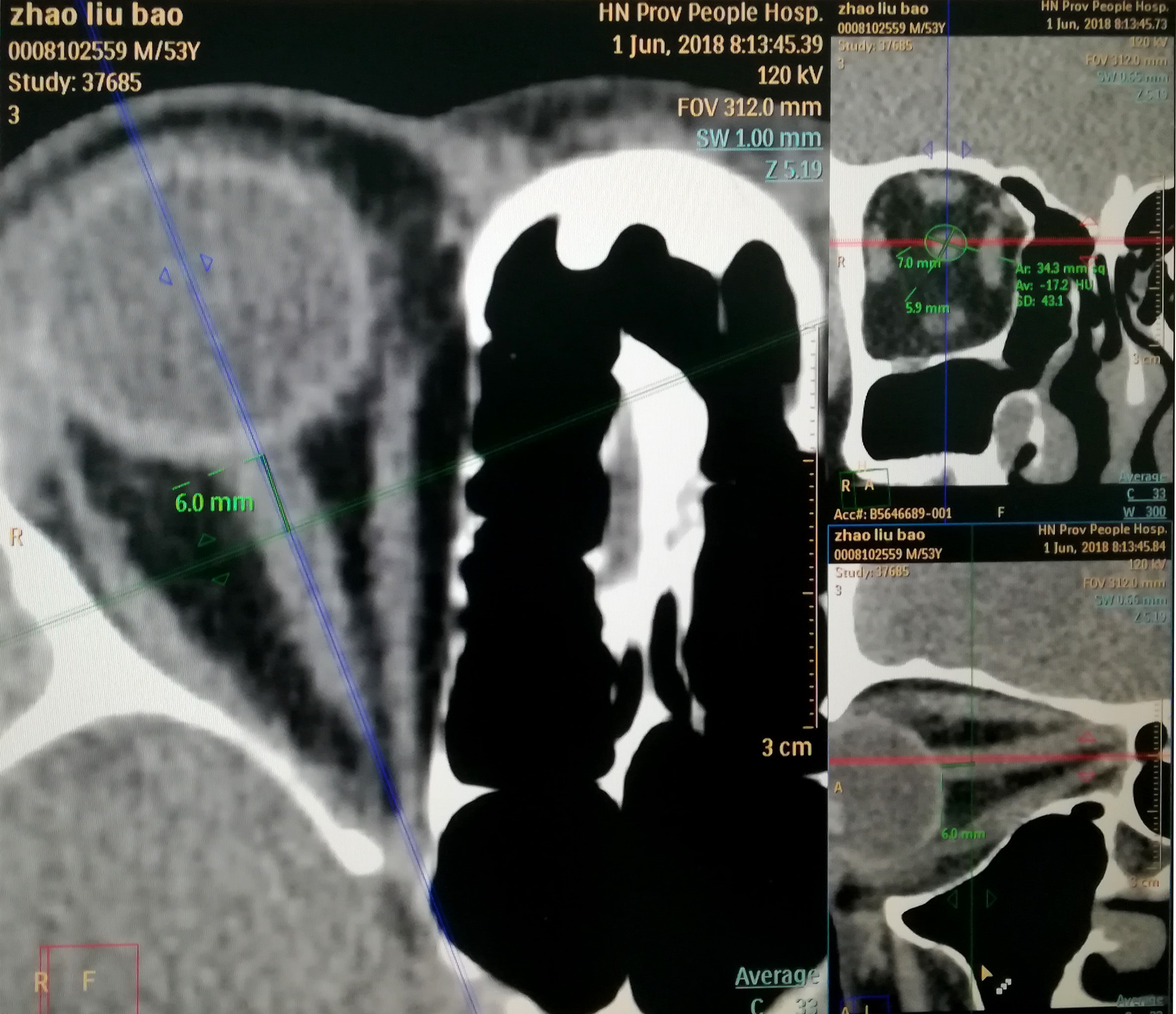
1.2 方法 采用Philips Brilliance 64层CT行颅脑容积扫描。受检查者仰卧,头正中位,闭合双眼。行颅脑1 mm层厚容积扫描,准直宽度为0.625 mm×64 mm,螺距1 mm,管电压120 kV,管电流400 mA,FOV为312 mm。选择健康眼图像清晰、噪声不明显的原始图像,传至Extended Brilliance Workspace V4.5.2图像后处理工作站。选择Advanced Vessel Analysis应用程序,从球后视神经起始处开始,沿着视神经走行,至视神经管入口附近为止,进行视神经的曲面重建处理。在视神经重建图像的冠状位分别选择距球后视神经起始部3、6、9、12 mm的点位,测量视神经横断面的最长径、最短径和面积(图1)。
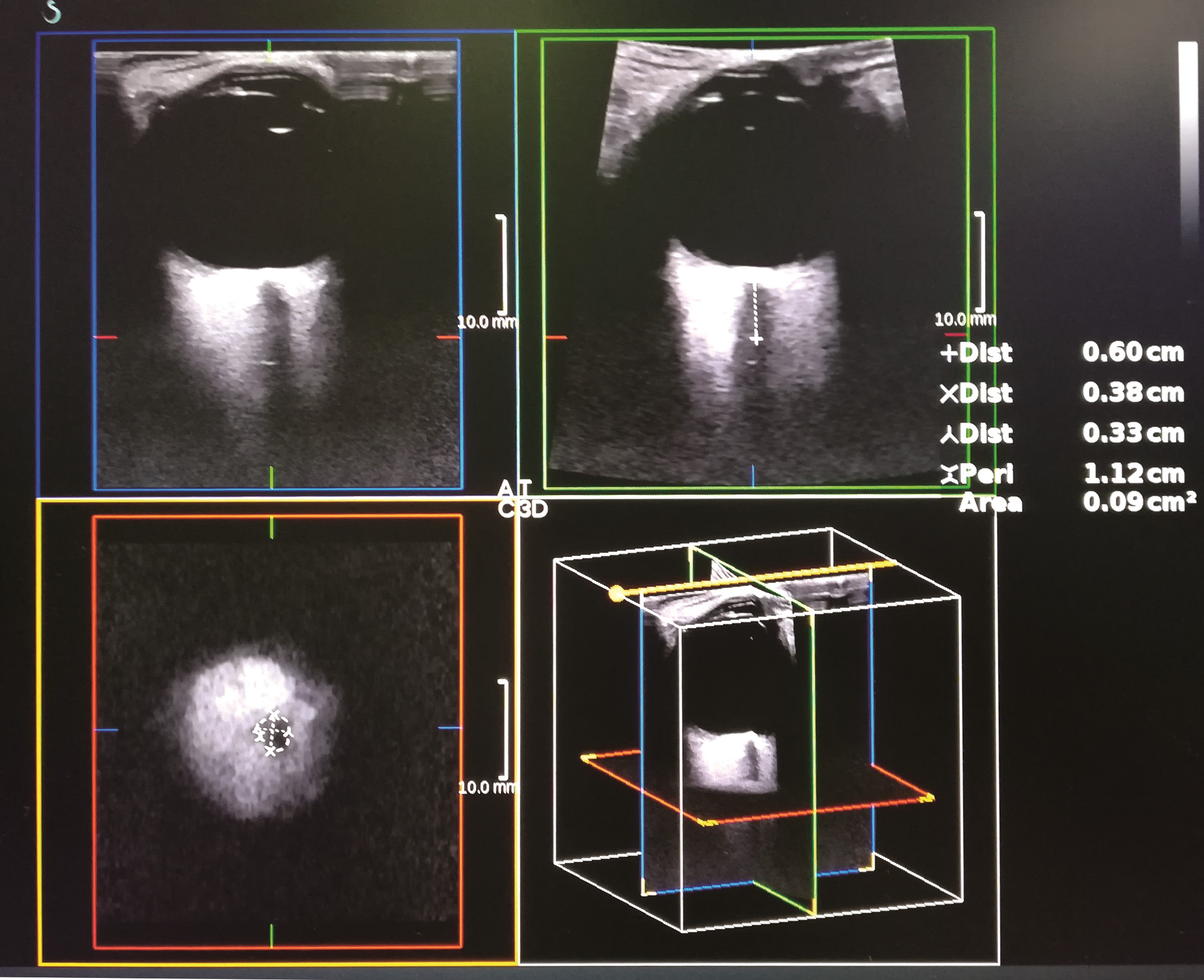
采用声科声红超声机器,高频三维超声探头扫查上述经CT扫描后的同一志愿者同一眼。受检查者仰卧,头保持正中,扫描时眼睑闭合,眼球瞳孔适当旋转至视神经清晰显示后保持眼球不动,启动三维成像模式获得图像,在视神经三维图像的冠状位分别选择距球后视神经起始部3、6、9、12 mm处,测量视神经横断面最长径、最短径及面积(图2)。检查时借鉴邱敬涛等[11]的操作将超声仪器输出功率调低,热指数(TI)和机械指数(MI)调至安全范围以下,检查时动作轻柔,避免对患者眼部压迫造成不必要的损害并尽量减少检查操作的时间。所有视神经的三维超声图像及参数由同一位检测者操作获得,所有视神经的CT后处理图像及参数由同一位检测者操作获得。
图1 多层螺旋CT扫描视神经重建图像,距球后视神经起始部6 mm点位视神经横断面的最长径、最短径和面积
Figure 1 The longest diameter,the shortest diameter and the area of the optic nerve cross section at the 6 mm point starting point of the retrobulbar optic nerve observed by multislice spiral CT scanning reconstruction
图2 三维超声视神经重建图像,距球后视神经起始部6 mm点位视神经横断面的最长径、最短径和面积
Figure 2 The longest diameter,the shortest diameter and the area of the optic nerve cross section at the 6 mm point starting point of the retrobulbar optic nerve observed by Three-dimensional ultrasonic imaging
1.3 统计学方法 采用SPSS 15.0统计学软件进行统计分析。测量参数经Kolmogorov-Smirnov检验呈正态分布,以均数±标准差(x±s)表示,组间方差经Levene检验方差齐。两种方式获得的距球后视神经起始部3、6、9、12 mm处各位点间视神经横断面最长径、最短径及面积的比较采用单因素方差分析,各位点间的多重比较采用SNK-q检验。两种方式获得的眶内段视神经横断面最长径、最短径及面积的比较采用独立样本t检验。P<0.05为差异有统计学意义。
2 结果
2.1 多层螺旋CT扫描后重建获得的距离球后视神经起始部不同距离处视神经横断面最长径、最短径及面积的变化 多层螺旋CT扫描后重建获得的距离球后视神经起始部3、6、9、12 mm位点视神经横断面长径的总体比较差异有统计学意义(F=214.218,P=0.001),各位点视神经横断面最长径两两比较差异均有统计学意义(P<0.05)。不同位点视神经横断面最短径总体比较差异有统计学意义(F=213.814,P=0.001),各位点视神经横断面最短径两两比较差异均有统计学意义(P<0.05)。不同位点视神经横断面面积比较差异有统计学意义(F=239.987,P=0.001),各位点视神经横断面面积两两比较差异均有统计学意义(P<0.05)。见表1。
表1 多层螺旋CT扫描后重建获得的距离球后视神经起始部不同距离处
视神经横断面最长径、最短径及面积比较 (x±s)
Table 1 Comparison of the longest diameter,shortest diameter and area of optic nerve transect at different distances from the initial distance of the retrobulbar optic nerve after multi-slice spiral CT reconstruction (x±s)
| 视神经与球后的距离(mm) |
n |
最长径(mm) |
最短径(mm) |
面积(mm2) |
| 3 |
102 |
6.13±0.39 |
5.52±0.47 |
27.28±3.82 |
| 6 |
102 |
5.35±0.45a |
4.89±0.43a |
22.13±3.24a |
| 9 |
102 |
5.10±0.39ab |
4.59±0.34ab |
19.24±2.81ab |
| 12 |
102 |
4.78±0.43abc |
4.36±0.29abc |
17.13±2.67abc |
| F值 |
|
214.218 |
213.814 |
239.987 |
| P值 |
|
0.001 |
0.001 |
0.001 |
注:与各自的3 mm位点值比较,aP<0.05;与各自的6 mm位点值比较,bP<0.05;与各自的9 mm位点值比较,cP<0.05
2.2 三维超声成像获得的距离球后视神经起始部不同距离处视神经横断面最长径、最短径及面积的变化 三维超声成像获得的距离球后视神经起始部3、6、9、12 mm位点视神经横断面长径的总体比较差异有统计学意义(F=237.325,P=0.001),各位点视神经横断面最长径两两比较差异均有统计学意义(均P<0.05)。不同位点视神经横断面最短径总体比较差异有统计学意义(F=219.763,P=0.001),各位点视神经横断面最短径两两比较差异均有统计学意义(均P<0.05)。不同位点视神经横断面面积比较差异有统计学意义(F=250.362,P=0.001),各位点视神经横断面面积两两比较差异均有统计学意义(均P<0.05)。见表2。
表2 三维超声成像获得的获得的距离球后视神经起始部不同距离处视神经横断面最长径、最短径及面积比较 (x±s)
Table 2 The longest distance,shortest diameter and area of optic nerve cross section at different distances from the initial part of the retrobulbar nerve were obtained by three-dimensional ultrasound imaging (x±s)
| 视神经与球后的距离(mm) |
n |
最长径(mm) |
最短径(mm) |
面积(mm2) |
| 3 |
102 |
6.38±0.32 |
5.65±0.37 |
27.49±4.12 |
| 6 |
102 |
5.65±0.37 |
4.95±0.29 |
23.08±3.73 |
| 9 |
102 |
5.01±0.31 |
4.47±0.31 |
18.54±2.65 |
| 12 |
102 |
4.65±0.27 |
4.35±0.37 |
17.43±3.07 |
| F值 |
|
237.325 |
219.763 |
250.362 |
| P值 |
|
0.001 |
0.001 |
0.001 |
注:与各自的3 mm位点值比较,aP<0.05;与各自的6 mm位点值比较,bP<0.05;与各自的9 mm位点值比较,cP<0.05
2.3 三维超声与多层螺旋CT扫描后重建获得的各位点横断面最长径、最短径及面积比较 三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部3 mm处横断面的最长径、最短径及面积比较差异均无统计学意义(t=1.805、P=0.074;t=1.930,P=0.056;t=1.329,P=0.187)。见表3。
表3 三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部
3 mm处横断面的最长径、最短径及面积比较 (x±s)
Table 3 Comparison of the longest diameter,shortest diameter and area at the 3 mm distance of the retrobulbar optic nerve after 3D ultrasound and multi-slice spiral CT reconstruction (x±s)
| 扫描方式 |
n |
最长径(mm) |
最短径(mm) |
面积(mm2) |
| 多层螺旋CT扫描后重建 |
102 |
6.13±0.39 |
5.52±0.47 |
27.28±3.82 |
| 三维超声 |
102 |
6.38±0.32 |
5.65±0.37 |
27.49±4.12 |
| t值 |
|
1.795 |
1.92 |
1.429 |
| P值 |
|
0.075 |
0.055 |
0.189 |
三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部6 mm处横断面的最长径、最短径及面积的比较差异均无统计学意义(t=0.724,P=0.471;t=1.562,P=0.121;t=1.424,P=0.158)。见表4。三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部9 mm处横断面的最长径、最短径及面积的比较差异均无统计学意义(t=0.724,P=0.471;t=1.562,P=0.121;t=1.424,P=0.158)。见表5。
三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部12 mm处横断面的最长径、最短径及面积的比较差异均无统计学意义(t=0.724,P=0.471;t=1.562,P=0.121;t=1.424,P=0.158)。见表6。
表4 三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部
6 mm处横断面的最长径、最短径及面积比较 (x±s)
Table 4 Comparison of the longest diameter,shortest diameter and area at the 6 mm distance of the retrobulbar optic nerve after 3D ultrasound and multi-slice spiral CT reconstruction (x±s)
| 扫描方式 |
n |
最长径(mm) |
最短径(mm) |
面积(mm2) |
| 多层螺旋CT扫描后重建 |
102 |
5.35±0.45 |
4.89±0.43 |
22.13±3.24 |
| 三维超声 |
102 |
5.65±0.37 |
4.95±0.29 |
23.08±3.73 |
| t值 |
|
1.815 |
1.831 |
1.349 |
| P值 |
|
0.077 |
0.056 |
0.177 |
表5 三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部
9 mm处横断面的最长径、最短径及面积比较 (x±s)
Table 5 Comparison of the longest diameter,shortest diameter and area at the 9 mm distance of the retrobulbar optic nerve after 3D ultrasound and multi-slice spiral CT reconstruction (x±s)
| 扫描方式 |
n |
最长径(mm) |
最短径(mm) |
面积(mm2) |
| 多层螺旋CT扫 |
102 |
5.10±0.39 |
4.59±0.34 |
19.24±2.81 |
| 三维超声 |
102 |
5.01±0.31 |
4.47±0.31 |
18.54±2.65 |
| t值 |
|
1.753 |
1.873 |
1.41 |
| P值 |
|
0.069 |
0.058 |
0.172 |
表6 三维超声与多层螺旋CT扫描后重建获得的距离球后视神经起始部
12 mm处横断面的最长径、最短径及面积 (x±s)
Table 6 The longest diameter,the shortest diameter and the area of the 12 mm distance from the initial part of the retrobulbar optic nerve were obtained after three-dimensional ultrasound and multi-slice spiral CT reconstruction (x±s)
| 扫描方式 |
n |
最长径(mm) |
最短径(mm) |
面积(mm2) |
| 多层螺旋CT扫 |
102 |
4.78±0.43 |
4.36士0.29 |
17.13±2.67 |
| 三维超声 |
102 |
4.65±0.27 |
4.35±0.37 |
17.43±3.07 |
| t值 |
|
1.675 |
1.912 |
1.342 |
| P值 |
|
0.078 |
0.061 |
0.151 |
3 讨论
由于视神经周围有硬脑膜、蛛网膜和软脑膜包围,其与颅内相应脑膜相延续等特点[12-13],眶内段视神经直径大小一定程度上可反映颅内压的变化[14-15]。基于此很多学者开展了眶内段视神经直径与颅内压关系的相关研究[16-17],取得很多成果。但迄今为止,眶内段视神经直径正常参考值和诊断颅内压增高的眶内段视神经直径标准还不统一[18-19];另外,关于种族、性别、年龄、个体特征、检查技术等多种因素对检测结果有何影响[20-21],仍需要大样本量进一步研究[22]。
由于多层螺旋CT能很快完成容积扫描成像,通过工作站后处理技术后可对眶内段视神经结构重建并检测其参数,操作简单,所以采用该方法测量正常人眶内段视神经横断面最长径、最短径和面积,结果发现,CT扫描重建后获得的各位点间视神经横断面的最长径、最短径及面积比较差异均有统计学意义,各位点视神经横断面最长径、最短径和面积两两比较差异均有统计学意义,正常人视神经随着与球后距离的延长,视神经逐渐变细,与以往的CT、磁共振及尸检等研究结果一致[23-24]。以往研究发现,距离球后视神经起始处3 mm处视神经的测量重复性较好[25-26],很多视神经直径研究也是以此位点做测量点[27-28],本次研究中多层螺旋CT重建测得距离球后视神经起始处3 mm处视神经鞘横断面最长径、最短径、横断面面积与游勇等[29]测量的结果相似,说明视神经CT重建横断面上进行参数测量获得的数据重复性较好,为以后正常视神经或异常视神经径线的测量奠定了一定的基础,有利于开展更多的关于视神经疾病的研究。
本次研究发现,三维超声成像获得的视神经数据分析结果与多层螺旋CT重建分析结果一致。三维超声成像获得的各位点间视神经横断面的最长径、最短径及面积比较差异均有统计学意义,各位点视神经横断面最长径、最短径和面积两两比较差异均有统计学意义,超声检查也发现正常人视神经随着与球后距离的延长,视神经逐渐变细。多层螺旋CT重建和三维超声成像获得的视神经各个参数无显著差异。说明两种技术在球后视神经横断面各参数测量方面没有差异,两者均可用于眶内段视神经方面的研究。部分基层医院无螺旋CT或一些特殊情况下,如需要床旁检测时,三维超声成像可以替代CT重建获得视神经参数,为进一步对视神经病变或视神经相关颅内病变的研究提供了一种有效、便利的工具[30-33]。
以往有学者采用普通超声对眶内段视神经参数进行研究,但所得到的眶内段视神经直径标准不统一。本次研究发现,三维超声成像获得的距离球后视神经起始处3 mm处视神经鞘横断面最短径与以往学者B型超声法[34-37]测量的结果类似,但此种结果不能绝对真实反映视神经的轮廓和外形[38-43],因三维超声成像和CT扫描后重建时均发现球后视神经横断面常呈椭圆形,单纯测量一个直径不能真实反映视神经的直径。三维超声成像和CT扫描后重建均能获得视神经鞘横断面的最长径、最短径及面积,能更真实反映视神经的轮廓和外形。
本次研究还发现,在距离球后12 mm以后更靠近颅内侧眶内段视神经的三维超声成像图像不清晰,与超声成像的声衰减及视神经走行弯曲形成侧方声影等伪像有关。但该段视神经在CT重建后的图像上可以清晰显示,可利用CT重建对该部位的视神经进行研究。总之,三维超声成像和CT扫描后重建在显示眶内段视神经方面都具有很多优势,两者均可以用来研究眶内段视神经,为研究眶内段视神经病变提供帮助。
4 参考文献
[1] MASCIOLI G,SALVOLINI S,CAVOLA G L,et al.Functional MRI examination of visual pathways in patients with unilateral optic neuritis[J/OL].Radiol Res Pract,2012,2012:265306[2015-05-11].http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3407659.doi:10.1155/2012/265306.
[2] WATANABE A,KINOUCHI H,HORIKOSHI T,et al.Effect of intracranial pressure on the diameter of the optic nerve sheath[J].J Neurosurg,2008,109(2):255-258.doi:10.3171/JNS/2008/109/8/0255.
[3] STRUMWASSER A,KWAN R O,YEUNG L,et al.Sonographic optic nerve sheath diameter as an estimate of intracranial pressure in adult trauma[J].J Surg Res,2011,170(2):265-271.doi:10.1016/j.jss.2011.03.009.
[4] REN R,ZHANG X,WANG N,et al.Cerebrospinal fluid pressure in ocular hypertention[J/OL].Acta Ophthalmol,2011,89(2):e142-148[2015-06-17].http://onlinelibrary.wiley.com/doi/10.1111/j.1755-3768.2010.02015.x.doi:10.1111/j.1755-3768.2010.02015.x.
[5] WANG N,XIE X,YANG D,et al.Orbital cerebrospinal fluid space in glaucoma:the Beijing intracranial and intraocular pressure(iCOP) study[J].Ophthalmology,2012,119:2 065-2 073.doi:10.1016/j.ophtha.2012.03.054.
[6] CHEN W W,WANG N,CAI S,et al.Structural brain abnormalities in patients with primary open-angle glaucoma:a study with 3T MR imaging[J].Invest Ophthalmol Vis Sci,2013,54(1):545-554.doi:10.1167/iovs.12-9893.
[7] WEIGEL M,LAGRZE W A,LAZZARO A,et al.Fast and quantitative high resolution magnetic resonance imaging of the optic nerve at 3.0 tesla[J].Invest Radiol,2006,41(2):83-86.
[8] 梁长虹,黄飚,黄美萍,等.视神经磁共振成像方法研究[J].现代临床医学生物工程学杂志,2002,8(3):191-200.
[9] 杨正汉,冯逢,王霄英,主编.磁共振成像技术指南[M].2版.北京:人民军医出版社,2010:58-161.
[10] 游勇,成洪波,樊宁,等.正常人眶内段视神经的CT重建和参数测量[J].中华实验眼科杂志,2015,33(11):1 015-1 018.
[11] 邱敬涛,甄艳华,卢学峰,等.高频超声测量视神经鞘直径在预测颅内压增高中的应用价值[J].中国实用神经疾病杂志,2018,21(3):297-300.
[12] KILLER H E,LAENG H R,FLAMMER J,et al.Architecture of arachnoid trabeculae,pillars,and septa in the subaraehnoid space of the human optic nerve:anatomy and clinical considerations[J].Br J Ophthalmol,2003,87(6):777-781.
[13] JONAS J B.Role of cerebrospinal fluid pressure in the pathogenesis of glaucoma[J].Acta Ophthalmol,2011,89(6):505-514.doi:10.1111/j.1755-3768.2010.01915.x.
[14] MORETTI R,PIZZI B.Ultrasonography of the optic nerve in neurocritically ill patients[J].Acta Anaes-thesiol Scand,2011,55(6):644-652.doi:10.1111/j.1399-6576.2011.02432.x.
[15] GEERAERTS T,MERCERON S,BENHAMOU D,et al.Non-invasive assessment of intracranial pressure using ocular sonography in neurocritical care patients[J].Intensive Care Med,2008,34(11):2 062-2 067.doi:10.1007/s00134-008-1149-x.
[16] MESSERER M,BERHOUMA M,MESSERER R.Interest of optic optic nerve sheath diameter ultrasonography in detecting non-invasively raised intracranial pressure[J].Neurochirurgie,2013,59(2):55-59.
[17] AMINI A,KARIMAN H,ARHAMI DOLATABADI A.Use of the sonographic diameter of optic nerve sheath diameter to estimate intracranial pressure[J].Am J Emerg Med,2013,31(1):236-239.
[18] DUBOURG J,JAVOU HEY E,GEERAERTS T,et al.Ultrasonography of optic nerve sheath diameter for de-tection of raised intracranial pressure:a systematic re-view and meta-analysis[J].Intensive Care Med,2011,37(7):1 059-1 068.
[19] KRISTIANSSON H,NISSBORG E,BARTEK J,et al.Measuring elevated intracranial pressure through non-invasive methods:a review of the literature[J].Neuro-surgAnesthesiol,2013,25(4):372-385.
[20] ORTIZ O,FLORES R A.Clinical and radiologic evaluation of the normal orbit[J].Semin Ultrasound,CT,MRI,1998,19:225-239.
[21] KARIM S,CLARK R A,POUKENS V,et al.Demonstration of systematic satiation in human intraorbital optic nerve size by quantitative magnetic resonance imaging and histology[J].Invest Ophthalmol Vis Sci,2004,45(4):1 047-1 051.
[22] LAGRZE W A,LAZZARO A,WEIGEL M.et al.Morphometry of the retrobulbar human optic nerve:comparison between conventional sonography and uhrafast magnetic resonance sequences[J].Invest Ophthalmol Vis Sci,2007,48(5):1 913-1 917.DOI:10.1167/iovs.06-1075.
[23] 刘津平,靳颖,李云生.视神经的断层解剖学研究及其临床意义[J].中国临床解剖学杂志,2003,21(5):454-456.
[24] 温生贵,张伟国,龚水根,等.正常成人眶内段视神经的MRI测量研究[J].实用放射学杂志,2000,16(9):556-559.
[25] 樊宁,成洪波,魏世辉,等.CT重建测量眶内段视神经的重复性研究[J].中华眼外伤职业眼病杂志,2014,36(5):336-339.
[26] BAUERLE J,LOCHNER P,KAPS M,et al.Intra-and interobsever reliability of sonographic assessment of the optic nerve sheathdiameter in healthy adults[J].J Neuroimaging,2012,22(1):42-45.dio:10.1111/j.1552-6569.2010.00546.x.
[27] 苗雨露,赵万,王福明,等.视神经鞘的超声解剖学研究[J].中国医药,2012,7(4):474-475.
[28] BRAFFMAN B H,NAIDICH T P,CHANELES M.Imaging anatomy of the normal orbit[J].Semin Ultrasound,CT,MRI,1997,18:403-412.
[29] 陈炽贤.实用放射学[M].北京:人民卫生出版社,1999:1 074-1 075.
[30] 苗雨露.超声检查视神经鞘直径监测颅内压的研究进展[J].海南医学,2014,25(19):2 882-2 884.
[31] 李世琪,李羽.超声测量视神经相关结构的变化在早期诊断颅内压增高中的应用[J].四川医学,2013,34(1):162-165.
[32] ARMSTRONG G T.LOCALIO A R,FEYGIN T,et al.Defining optic nerve tortuosity[J].Am J Neu roradio1.2007,28(4):666-671.
[33] GRONEMEYER S A,LANGSTON J W,ABRAHAM J.Curved reconstruction along the anterior optic pathway[J].Am J Neuroradiol,1998,19(2):338-340.
[34] 齐燕,陈楠,王星,等.高分辨率MR测量国人正常成年男性视神经长度[J].中国医学影像技术,2010,26(5):840-843.
[35] 毛青,王培军,包颜明,等.MRI与解剖对比研究:视神经-眼平面脑外段视神经的表现[J].医学影像学杂志,2008,18(8):821-822.
[36] XIA Z R,YING J L,ZHANG J,et al.Macular and retinal nerve fiber layer thickness in myopic children by three-dimensional OCT[J].Zhonghua Yi Xue Za Zhi,2013,93(45):3 573-3 576.
[37] ZEILER F A,UNGER B,KRAMER A H,et al.A unique model for ultrasound assessment of optic nerve sheath diameter[J].Can J Neurol Sci,2013,40(2):225-229.
[38] AN L,JOHNSTONE M,WANG R K.Optical microangiography provides correlation between microstructure and microvasculature of optic nerve head in human subjects[J].J Biomed Opt,2012,17(11):116 018.
[39] BROVKINA A F,IATSENKO O I.Is differential diagnosis between soft tissue paraneural lesions and optic nerve tumors using computer tomography possible?[J].Vestn Oftalmol,2010,126(6):29-32.
[40] BAULT J P,SALOMON L J,GUIBAUD L,et al.Role of three-dimensional ultrasound measurement of the optic tract in fetuses with agenesis of the septum pellucidum[J].Ultrasound Obstet Gynecol,2011,37(5):570-575.
[41] ZHIHAI L,QIXUE G,BAOHONG T,et al.Three-dimensional reconstruction of the optic canal-based on multislice helical CT:a comparison analysis with skull dissection of 40 postmortem cases[J].Anat Rec (Hoboken),2008,291(12):1 662-1 672.
[42] LI Z,GAO Q,CAL Z,et al.Three dimensional reconstruction study of multi-slice helical CT imaging on optic canal area[J].Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi,2007,21(1):7-9.
[43] BAULT J P.Visualization of the fetal optic chiasma using three-dimensional ultrasound imaging[J].Ultrasound Obstet Gynecol,2006,28(6):862-864.
(收稿2018-06-01 修回2018-07-10)
本文引用信息:刘银龙,吴刚,孔莎,罗帅伟,朱丽敏.三维超声与多层螺旋CT扫描重建在正常人眶内段视神经的参数测量及对比研究[J].中国实用神经疾病杂志,2018,21(18):1978-1985.DOI:10.12083/SYSJ.2018.18.439
Reference information:LIU Yinlong,WU Gang,KONG Sha,LUO Shuaiwei,ZHU Limin.Parametric measurement and comparative study of three-dimensional ultrasound and multi-slice spiral CT reconstruction in the optic nerve of normal human sacral[J].Chinese Journal of Practical Nervous Diseases,2018,21(18):1978-1985.DOI:10.12083/SYSJ.2018.18.439