目的 探讨蛛网膜下腔出血(SAH)患者脑脊液(CSF)中白细胞介素-6(IL-6)及其他生物标记对早期诊断脑血管痉挛及脑室炎的价值。方法 选取80例SAH患者为研究对象,自脑室外引流中获取CSF并分离相关的血清生物标记物,通过曲线下面积(AUC)、截止值、敏感度与特异性评估各标记物与脑血管痉挛、脑室炎及并发症的关系。结果 33例患者发生脑血管痉挛,21例发生脑室炎,26例为单纯SAH,3组IL-6水平分别为(7 621±4 438)pg/mL、(4 117±4 652)pg/mL、(244.9±24
蛛网膜下腔出血颅内血管痉挛及炎症的相关标记物探讨
曲良卓
开封市中心医院检验科,河南 开封 475000
作者简介:曲良卓,Email:lixin7607@163.com
【摘要】 目的 探讨蛛网膜下腔出血(SAH)患者脑脊液(CSF)中白细胞介素-6(IL-6)及其他生物标记对早期诊断脑血管痉挛及脑室炎的价值。方法 选取80例SAH患者为研究对象,自脑室外引流中获取CSF并分离相关的血清生物标记物,通过曲线下面积(AUC)、截止值、敏感度与特异性评估各标记物与脑血管痉挛、脑室炎及并发症的关系。结果 33例患者发生脑血管痉挛,21例发生脑室炎,26例为单纯SAH,3组IL-6水平分别为(7 621±4 438)pg/mL、(4 117±4 652)pg/mL、(244.9±240.5)pg/mL(P<0.001);CSF内IL-6水平能够很好地评估区分脑室炎及单纯SAH(AUC 1.00,截止值707 pg/mL,敏感度100%,特异性100%),而区分脑血管痉挛与脑室炎的潜力为中等。血管痉挛患者CSF中IL-6水平显著高于单纯SAH患者。结论 SAH患者发生脑血管痉挛或脑室炎时CSF的IL-6水平明显升高,可通过截止值确定具体的并发症类型,以辅助指导及早给予临床干预。
【关键词】 蛛网膜下腔出血;脑室炎;脑血管痉挛;标记物;脑脊液;血清
【中图分类号】 R743.35 【文献标识码】 A 【文章编号】 1673-5110(2018)19-2165-06 DOI:10.12083/SYSJ.2018.19.470
Discussion on related markers of intracranial vasospasm and inflammation in subarachnoid hemorrhage
QU Liangzhuo
Department of Clinical Laboratory,Kaifeng Central Hospital,Kaifeng 475000,China
【Abstract】 Objective To investigate the value of interleukin-6 (IL-6) and other biomarkers in cerebrospinal fluid (CSF) in patients with subarachnoid hemorrhage (SAH) for early diagnosis of cerebral vasospasm and ventriculitis.Methods Eighty patients with SAH were enrolled in the study.CSF was obtained from extraventricular drainage and related serum biomarkers were isolated.The markers and cerebral vasospasm were evaluated by area under the curve (AUC),cutoff,sensitivity and specificity.The relationship between ventriculitis and complications.Results 33 patients developed cerebral vasospasm,21 patients developed ventriculitis,26 patients were treated with SAH alone,and the average IL-6 levels in the 3 groups were (7 621±4 438) pg/mL,(4 117±4 652) pg/mL,(244.9 ±240.5) pg/mL (P<0.001);IL-6 levels in CSF can be well assessed to distinguish between ventriculitis and SAH alone (AUC 1.00,cut-off 707 pg/mL,sensitivity 100%,specificity 100%) And the potential to distinguish between cerebral vasospasm and ventriculitis is moderate.IL-6 levels in CSF were significantly higher in patients with vasospasm than in patients with SAH alone.Conclusion The level of IL-6 in CSF is significantly increased in patients with SAH after cerebral vasospasm or ventriculitis.The specific type of complications can be determined by cut-off value to assist in early clinical intervention.
【Key words】 Subarachnoid hemorrhage;Ventricular inflammation;Cerebral vasospasm;Marker;Cerebrospinal fluid;Serum
动脉瘤性蛛网膜下腔出血是神经外科的常见急症之一,脑血管痉挛及颅内感染可显著增加发病率及病死率[1-3]。研究显示,红细胞进入蛛网膜下腔及其后产生的裂解能够激活机体的免疫反应,增加CSF内的促炎症细胞因子水平,其可使患者临床预后恶化[4-5]。因此,本研究探讨IL-6及其他生物因子对脑室炎的诊断价值,并与单纯SAH患者的分子水平进行对比研究。
1 资料与方法
1.1 研究对象 选取2014-01—2016-12治疗的80例SAH患者为研究对象,依据Fisher分级及世界神经外科医师联盟(WFNS)分级系统对SAH的严重程度进行评估[6-7];通过CT、MRI及数字减影全脑血管造影(DSA)等检查手段确认出血点并进行相应血管夹闭等干预治疗。
1.2 血清及CSF生物标记物 脑室外引流的适应证为脑室内出血及脑积水和(或)不可评估的神经功能状态,放置引流管前静脉给予头孢呋辛抗生素预防。通过三通旋塞在严格无菌操作下抽取CSF样本,按照SAH常规诊疗,每日监测CSF内的IL-6、C反应蛋白及白细胞计数,每周2次监测血清降钙素原水平,或伴细菌感染或败血症则增加检测的频率。
1.3 脑血管痉挛及脑室炎的定义 脑室炎定义为CSF培养显示存在阳性微生物,临床存在感染的征象;葡萄糖水平<40 mg/dL或<50%血清葡萄糖水平;CSF蛋白水平升高(>50 mg/dL);CSF细胞数异常增多(100个/mm3);CSF革兰染色阳性。脑血管痉挛符合以下3个标准中的至少1项:(1)新出现的神经损害;(2)经颅多普勒超声检查示大脑中动脉或前动脉血流速度>120 cm/s,Lindegaard指数阳性,大脑中动脉与颈内动脉血流比值>3;(3)影像学检查存在脑血管痉挛。
1.4 统计学方法 采用SPSS 20.0软件,受试者工作特征曲线及曲线下面积用于评价每个生物标记物的诊断潜能;Youden J统计用于获得最大灵敏度与特异性的截止值;主要结果参数为阳性似然比(+LR)、阴性似然比(-LR)、敏感度及特异性;P<0.05为差异有统计学意义。
2 结果
2.1 患者基本信息 本组患者年龄(56.5±13.8)岁,男女比例为23∶17;79例患者出血原因为动脉瘤,其中10例存在动静脉的畸形;33例出现脑血管痉挛[出血后(5.8±4.4)d];WFNS分级≥IV与脑血管痉挛的发生显著相关(P<0.01);21例出现脑室炎[出血后(7.6±3.0)d];26例内未发现脑室炎与脑血管痉挛,为单纯SAH患者。
2.2 脑室炎与脑血管痉挛的生物标记物 首次诊断时脑室炎与脑血管痉挛前患者的CSF内IL-6含量分别(7 621±4 438)pg/mL、(4 117±4 652) pg/mL(P=0.66),显著高于单纯SAH患者的(244.9±240.5)pg/mL(P<0.01);脑室炎的AUC为0.847,截止值为3 200 pg/mL(敏感度86.4%,特异性83.6%,+LR 4.7,-LR 0.20)。
脑室内的IL-6对鉴别脑室炎与单纯SAH具有非常优秀的诊断潜能(AUC 1.00,截止值712 pg/mL,敏感度100%,特异性100%,+LR ∞,-LR 0);脑血管痉挛患者CSF中IL-6水平显著高于单纯SAH出血患者(AUC 0.868,截止值540 pg/mL,敏感度88.0%,特异性92.1%,+LR 11.2,-LR 0.17);区分脑室炎与脑血管痉挛的诊断潜能为中度(AUC 0.766,截止值3 200 pg/mL,敏感度85.2%,特异性68.4%,+LR 2.7,-LR 0.16)(图1);血清IL-6分子表达对鉴别脑室炎与血管痉挛(P=0.66)或与单纯SAH无显著差异(P=0.98);CSF与血清IL-6含量比值在引流相关感染病例内显著高于单纯SAH者(P=0.003),而与脑室炎患者无显著性差异(P=0.12,表1)。
脑室炎患者CSF内多形核细胞百分比与单纯出血患者相比亦显著升高(P=0.04),显著高于脑血管痉挛患者(P=0.03);血清C反应蛋白无显著性差异,其他参数与病情进展未见显著性关联(表1)。
表1 血清与CSF标记物对脑室炎的诊断潜能评价
Table 1 Evaluation of the diagnostic potential of serum and CSF markers for ventriculitis
| 项目 |
CSF多形细胞百分比/% |
CSF与血清IL-6比值 |
血清IL-6 (pg/mL) |
血清CRP (mg/dL) |
| AUC(95% CI) |
0.772(0.645~0.948) |
0.796(0.638~0.945) |
0.585(0.408~0.775) |
0.667(0.532~0.887) |
| 截止值 |
65 |
55.8 |
11.2 |
5.9 |
| 敏感度(95% CI) |
83.7(56.2~94.2) |
87.5(60.3~97.2) |
100(87.6~100) |
59.4(37.6~80.4) |
| 特异性(95% CI) |
75.2(48.3~83.5) |
66.5(48.0~83.3) |
23.2(10.0~38.7) |
76.5(60.3~88.7) |
| 阳性似然比(95% CI) |
2.6(1.25~4.78) |
2.7(1.44~4.99) |
1.33(1.14~1.76) |
2.44(1.18~5.03) |
| 阴性似然比(95% CI) |
0.21(0.09~0.79) |
0.18(0.07~0.82) |
0 |
0.50(0.34~1.05) |
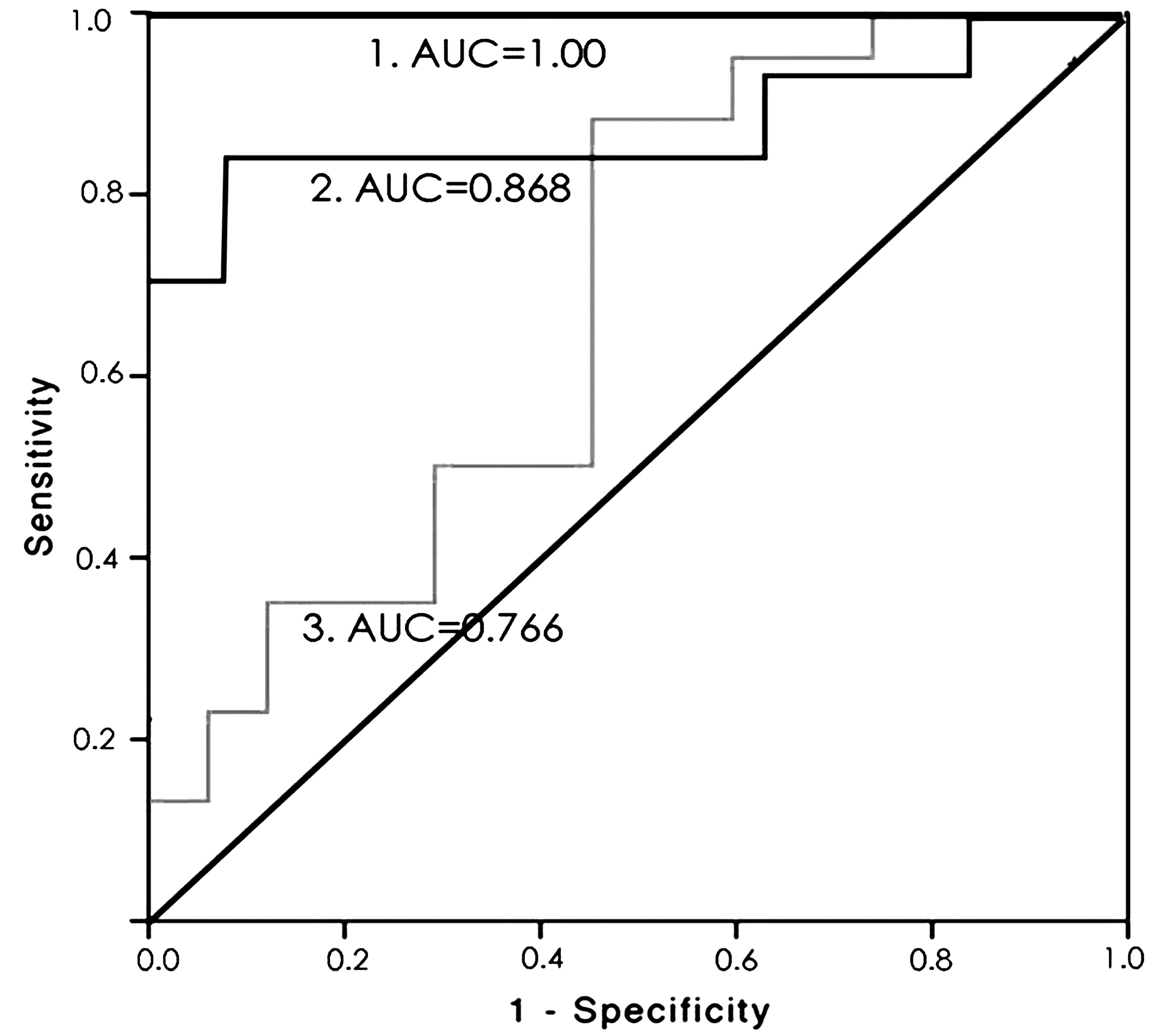
图1 CSF IL-6鉴别,脑室炎与单纯SAH、脑血管痉挛与单纯SAH、脑室炎与脑血管痉挛的临床诊断潜能比较
Figure 1 Comparison of clinical diagnosis potential of CSF IL-6,ventricular inflamma-tion and simple SAH,cerebral vasospasm and simple SAH,ventriculitis and cerebral vasospasm
3 讨论
严重SAH患者通常处于插管及昏迷状态,临床表现及神经损害评估对预测具体的病理进展程度的作用十分有限[8-14]。由于脑室外引流相关的感染概率可增加约27%,抗生素的预防使用往往使革兰染色与细菌培养的阳性率降低[15-20]。文献报道SAH伴脑血管痉挛发生概率可达47%左右,然而可能受不同诊断标准影响,不同研究间的可比性有限[5-6,21-30]。本研究中脑血管痉挛的发生率为42.9%,且其与Fisher分级、患者临床预后较差相关。
本研究主要目的在于评价血清和CSF内可溶性炎症生物标记物与脑室炎、脑血管痉挛早期诊断的相关性,其中重点评价了IL-6分子的表达,原因为目前大量的文献均报道其与颅内出血、脑外伤、脑膜炎等多种病变相关[31-40]。研究发现,IL-6的表达水平在SAH患者中显著升高,根据其相关的截止值还可有效对患者的脑血管痉挛与脑室炎进行区分,这与文献中的观点一致[41-43]。除此还发现,CSF与血清IL-6水平的比值与单独的CSF内IL-6水平相比并不能提高诊断的准确性,血清IL-6与CRP分子水平无法进一步评价患者病情的进展,分析原因可能为脑室炎为局部区域的炎症反应,对机体整个系统的影响性较小[44-49]。
除IL-6分子外,CSF内的多形核细胞百分比在脑室炎患者内显著升高,诊断的可靠性为中等,主要由于脑出血后红细胞在CSF内降解[50-51]。研究报道[52-57],多形细胞百分比对评价神经外科手术后脑膜炎的敏感性为94%,特异性为28%;研究显示,多形细胞百分比能够有效鉴别细菌性与坏死性脑膜炎[58-60]。因此,此参数可较好地辅助临床相关诊断,其中包括脑室外引流相关的脑室炎。
本研究初步证实,SAH患者发生脑血管痉挛或脑室炎时CSF内IL-6水平明显升高,可通过截止值确定具体的并发症类型,以辅助指导及早给予临床干预。
4 参考文献
[1] FILIPCE V,CAPAROSKI A.The Effects of Vasospasm and Re-Bleeding on the Outcome of Patients with Subarachnoid Hemorrhage from Ruptured Intracranial Aneurysm[J].Pril (Makedon Akad Nauk Umet Odd Med Nauki),2015,36(3):77-82.doi:10.1515/prilozi-2015-0081.
[2] DURRANT J C,HINSON H E.Rescue therapy for refractory vasospasm after subarachnoid hemorrhage[J].Curr Neurol Neurosci Rep,2015,15(2):521.doi:10.1007/s11910-014-0521-1.
[3] WU W,GUAN Y,ZHAO G,et al.Elevated IL-6 and TNF-α Levels in Cerebrospinal Fluid of Subarachnoid Hemorrhage Patients[J].Mol Neurobiol,2015,53(5):1-9.
[4] DASTYCH M,GOTTWALDOVÁ J,CERMÁKOVÁ Z.Calprotectin and lactoferrin in the cerebrospinal fluid;biomarkers utilisable for differential diagnostics of bacterial and aseptic meningitis?[J].Clin Chem Lab Med,2014,53(4):599-603.
[5] 刘永飞,赵贵锋.动脉瘤蛛网膜下腔出血后脑血管痉挛药物治疗的研究进展[J].医学综述,2016,22(13):2 607-2 612.
[6] MILLER B A,TURAN N,CHAU M,et al.Inflammation,vasospasm,and brain injury after subarachnoid hemorrhage[J].Biomed Res Int,2014,2014:384342.doi:10.1155/2014/384342.
[7] BILLINGSLEY J T,HOH B L.Vasospasm in aneury-smal subarachnoid hemorrhage[J].World Neurosurg,2014,82(3/4):250-252.doi:10.1016/j.wneu.2014.06.048.Epub 2014 Jun 28.PubMed PMID:24984246.
[8] JONES J,SAYRE J,CHANG R,et al.Cerebral vasospasm patterns following aneurysmal subarachnoid hemorrhage:an angiographic study comparing coils with clips[J].J Neurointerv Surg,2015,7(11):803-807.
[9] 康志新.蛛网膜下腔出血患者头痛发作时经颅多普勒超声监测指标变化的临床研究[J].中国医药导报,2017,14(20):94-96.
[10] 王翊飞,张李涛,褚正民,等.前列地尔注射液联合尼莫地平注射液治疗动脉瘤性蛛网膜下腔出血伴脑血管痉挛的临床研究[J].中国临床药理学杂志,2016,32(21):1 942-1 945.
[11] RASMUSSEN R,WETTERSLEV J,STAVNGAARD T,et al.Effects of prostacyclin on cerebral blood flow and vasospasm after subarachnoid hemorrhage:randomized,pilot trial[J].Stroke,2015,46(1):37-41.
[12] WILSON C D,SHANKAR J J.Diagnosing Vasospasm After Subarachnoid Hemorrhage:CTA and CTP[J].Can J Neurol Sci,2014,41(3):314-349.
[13] 姜涛,周杰,周水晶,等.芳香开窍药嗅吸剂联合尼莫地平对创伤性蛛网膜下腔出血后脑血管痉挛的影响[J].中医杂志,2015,56(6):492-495.
[14] NAIDECH A,DU Y,KREITER K T,et al.Dobuta-mine versus milrinone after subarachnoid hemorrhage[J].Neurosurgery,2016,56(1):26-27.
[15] CIUREA A V,PALADE C,VOINESCU D,et al.Subarachnoid hemorrhage and cerebral vasospasm-literature review[J].J Med Life,2013,6(2):120-125.
[16] LENSKI M,BICZOK A,HUGE V,et al.Role of Cerebrospinal Fluid Markers for Predicting Shunt-Depen-dent Hydrocephalus in Patients with Subarachnoid Hemorrhage and External Ventricular Drain Placement[J].World Neurosurg,2018 Sep 27.doi:10.1016/j.wneu.2018.09.159.
[17] LINDGREN C,KOSKINEN L O,SSOZI R,et al.Cerebrospinal fluid lactate and neurological outcome after subarachnoid haemorrhage[J].J Clin Neurosci,2018 Oct 22.doi:10.1016/j.jocn.2018.10.025.
[18] JABBARLI R,PIERSCIANEK D,DARKWAH OPPONG M,et al.Laboratory biomarkers of delayed cerebral ischemia after subarachnoid hemorrhage:a systematic review[J].Neurosurg Rev,2018 Oct 10.doi:10.1007/s10143-018-1037-y.
[19] AYAZ M,YANARDAG S B.SAH-Induced Electrophysiological Changes of Ventricular Myocytes and Role of N-acetylcysteine Protection[J].J Neurol Surg A Cent Eur Neurosurg,2018 Oct 31.doi:10.1055/s-0038-1655739.
[20] CHENG Y W,LI W J,DOU X J,et al.Role of endothelin-1 and its receptors in cerebral vasospasm following subarachnoid hemorrhage[J].Mol Med Rep,2018 Sep 27.doi:10.3892/mmr.2018.9513.
[21] HE T,ZUO Y,AI-ZAKWANI K,et al.Subarachnoid hemorrhage enhances the expression of TDP-43 in the brain of experimental rats and human subjects[J].Exp Ther Med,2018,16(4):3 363-3 368.doi:10.3892/etm.2018.6636.
[22] WANG K C,TANG S C,LEE J E,et al.Impaired microcirculation after subarachnoid hemorrhage in an in vivo animal model[J].Sci Rep,2018,8(1):13 315.doi:10.1038/s41598-018-31709-7.
[23] ZHANG W,SUN L,MA L,et al.Clinical significance of changes in IL-6,CRP and S100in serum and NO in cerebrospinal fluid insubarachnoid hemorrhage and prognosis[J].Exp Ther Med,2018,16(2):816-820.doi:10.3892/etm.2018.6231.
[24] THOMAS A J,OGILVY C S,GRIESSENAUER C J,et al.Macrophage CD163 expression in cerebrospinal fluid:association with subarachnoid hemorrhage outcome[J].J Neurosurg,2018,20:1-7.doi:10.3171/2018.2.JNS172828.
[25] BUUNK A M,GROEN R J M,WIJBENGA R A,et al.Mental versus physical fatigue after subarachnoid hemorrhage:differential associations with outcome[J].Eur J Neurol,2018,25(11):1313-e113.doi:10.1111/ene.13723.
[26] VINAS RIOS J M,SANCHEZ-AGUILAR M,KRETS-CHMER T,et al.Predictors of hydrocephalus as a complication of non-traumatic subarachnoid hemorrhage:a retrospective observational cohort study in 107 patients[J].Patient Saf Surg,2018,12:13.doi:10.1186/s13037-018-0160-6.
[27] SONG Y,LIM B J,KIM D H,et al.Effect of Dexmedetomidine on Cerebral Vasospasm and Associated Biomarkers in a Rat Subarachnoid Hemorrhage Model[J].J Neurosurg Anesthesiol,2018 Apr 20.doi:10.1097/ANA.0000000000000504.
[28] BORKAR S A,SINGH M,KALE S S,et al.Spinal Cerebrospinal Fluid Drainage for prevention of Vasospasm in Aneurysmal Subarachnoid Hemorrhage:A Prospective,Randomized controlled study[J].Asian J Neurosurg,2018,13(2):238-246.doi:10.4103/1793-5482.228512.
[29] KIM W,LEE S H,AHN Y J,et al.A label-free cellulose SERS biosensor chip with improvement of nanoparticle-enhanced LSPR effects for early diagnosis of subarachnoid hemorrhage-induced complications[J].Biosens Bioelectron,2018,111:59-65.doi:10.1016/j.bios.2018.04.003.
[30] LIU J P,YE Z N,LV S Y,et al.The rise of soluble platelet-derived growth factor receptor β in CSF early after subarachnoid hemorrhage correlates with cerebral vasospasm[J].Neurol Sci,2018,39(6):1 105-1 111.doi:10.1007/s10072-018-3329-y.
[31] CHEN J,CHEN G,LI J,et al.Melatonin attenuates inflammatory response-induced brain edema in early brain injury following a subarachnoid hemorrhage:a possible role for the regulation of pro-inflammatory cytokines[J].J Pineal Res,2015,57(3):340-347.
[32] FUJIMURA M,JOO J Y,KIM J S,et al.Preventive Effect of Clazosentan against Cerebral Vasospasm after Clipping Surgery for Aneurysmal Subarachnoid Hemorrhage in Japanese and Korean Patients[J].Cerebrovasc Dis,2017,44(1/2):59-67.doi:10.1159/000475824.
[33] MIJITI M,MIJITI P,AXIER A,et al.Incidence and Predictors of Angiographic Vasospasm,Symptomatic Vasospasm and Cerebral Infarction in Chinese Patients with Aneurysmal Subarachnoid Hemorrhage[J].PLoS One,2016,11(12):e0168657.doi:10.1371/journal.pone.0168657.
[34] RAO G S,MUTHUCHELLAPPAN R.Cerebral vasospasm:current understanding[J].Curr Opin Anaesthesiol,2016,29(5):544-551.doi:10.1097/ACO.0000000000000370.
[35] SCHUSS P,HADJIATHANASIOU A,BRANDECK-ER S,et al.Risk factors for shunt dependency in patients suffering from spontaneous,non-aneurysmal subarachnoid hemorrhage[J].Neurosurg Rev,2018 Mar 29.doi:10.1007/s10143-018-0970-0.
[36] ASCANIO L C,GUPTA R,ADEEB N,et al.Relation-ship between external ventricular drain clamp trials and ventriculoperitoneal shunt insertion following nontraumatic subarachnoid hemorrhage:a single-center study[J].J Neurosurg,2018,16:1-7.doi:10.3171/2017.10.JNS171644.
[37] KOYANAGI M,FUKUDA H,SAIKI M,et al.Effect of choice of treatment modality on the incidence of shunt-dependent hydrocephalus after aneurysmal subarachnoid hemorrhage[J].J Neurosurg,2018,9:1-7.doi:10.3171/2017.9.JNS171806.
[38] CHEN Y A,WANG K C,LIU D Z,et al.The Proliferation Capacity of Cultured Neural Stem Cells Promoted by CSF Collected from SAH Patients Correlates to Clinical Outcome[J].Sci Rep,2018,8(1):1 109.doi:10.1038/s41598-018-19371-5.
[39] NOGUEIRA A B,NOGUEIRA A B,VEIGA J C E,et al.Hypothesis on the Role of Cryptochromes in Inflammation and Subarachnoid Hemorrhage Outcome[J].Front Neurol,2017,8:637.doi:10.3389/fneur.2017.00637.
[40] HALAWA I,VLACHOGIANNIS P,AMANDUSSON ,et al.Seizures,CSF neurofilament light and tau in patients with subarachnoid haemorrhage[J].Acta Neurol Scand,2018,137(2):199-203.doi:10.1111/ane.12873.
[41] HAMMER C,DAOU B,CHALOUHI N,et al.Decreased CSF output as a clinical indicator of cerebral vasospasm following aneurysmal subarachnoid hemorrhage[J].Clin Neurol Neurosurg,2016,144:101-104.doi:10.1016/j.clineuro.2016.03.024.
[42] EGASHIRA Y,ZHAO H,HUA Y,et al.White matter injury after subarachnoid hemorrhage:role of blood-brain barrier disruption and matrix metalloproteinase-9[J].Stroke,2015,46(10):2 909-2 915.
[43] 杨波,丁文学,尚爱加,等.动脉瘤介入术后予尼莫地平动脉内灌注治疗蛛网膜下腔出血后脑血管痉挛的临床研究[J].临床和实验医学杂志,2017,16(8):768-771.
[44] 高建亮,张中原,张小章,等.大鼠SAH后学习记忆改变与炎症反应的相关性[J].河北医科大学学报,2018,39(9):1 073-1 076.
[45] 陈朝晖,洪溪屏,兰频,等.TTP减轻大鼠蛛网膜下腔出血后早期脑损伤[J].中国病理生理杂志,2018,34(2):287-293.
[46] 陈功,陈祥,朱丹丹,等.体外模拟SAH状况下IL-6对大鼠蛛网膜细胞极化状态的影响[J].浙江医学,2018,40(10):1 027-1 032,后插1.
[47] 行治国,赵君杰,宋锦宁,等.星型胶质细胞代谢抑制剂氟代柠檬酸对大鼠蛛网膜下腔出血的保护作用及机制[J].西安交通大学学报(医学版),2018,39(4):530-536.
[48] 周刚,王佳君.亚低温治疗联合尼莫地平脑池内灌注治疗蛛网膜下腔出血后脑血管痉挛的临床疗效[J].心血管康复医学杂志,2018,27(3):289-293.
[49] 徐艳,张晓珺,任红.红景天对蛛网膜下腔出血后脑血管痉挛大鼠炎症介质水平及血管内皮功能的影响[J].中国医师杂志,2018,20(2):238-242.
[50] SHAO A,WU H,HONG Y,et al.Hydrogen-Rich Saline Attenuated Subarachnoid Hemorrhage-Induced Early Brain Injury in Rats by Suppressing Inflamma-tory Response:Possible Involvement of NF-κB Pathway and NLRP3 Inflammasome[J].Mol Neurobiol,2016,53(5):1-15.
[51] GRIESSENAUER C J,CHUA M H,HANAFY K A,et al.Soluble Fms-Like Tyrosine Kinase 1 (sFlt-1) and Risk of Cerebral Vasospasm After Aneurysmal Subarachnoid Hemorrhage[J].World Neurosurg,2017,108:84-89.doi:10.1016/j.wneu.2017.08.128.
[52] MA Y,QIAO G,YIN Y,et al.Protective Effects of Astragaloside IV on Delayed Cerebral Vasospasm in an Experimental Rat Model of Subarachnoid Hemorrhage[J].World Neurosurg,2018,118:e443-e448.
[53] CHAUDHRY S R,STOFFEL-WAGNER B,KINFE T M,et al.Elevated Systemic IL-6 Levels in Patients with Aneurysmal Subarachnoid Hemorrhage Is an Unspecific Marker for Post-SAH Complications[J].Int J Mol Sci,2017,18(12).doi:10.3390/ijms18122580.
[54] DURI K,NEUMAN E,VYBÍHAL V,et al.Early Dynamics of Interleukin-6 in Cerebrospinal Fluid after Aneurysmal Subarachnoid Hemorrhage[J].J Neurol Surg A Cent Eur Neurosurg,2018,79(2):145-151.
[55] LI Y,SUN F,JING Z,et al.Glycyrrhizic acid exerts anti-inflammatory effect to improve cerebral vasospasm secondary to subarachnoid hemorrhage in a rat model[J].Neurol Res,2017,39(8):727-732.
[56] LENSKI M,HUGE V,BRIEGEL J,et al.Interleukin 6 in the Cerebrospinal Fluid as a Biomarker for Onset of Vasospasm and Ventriculitis After Severe Subarachn-oid Hemorrhage[J].World Neurosurg,2017,99:132-139.
[57] CROCI D,NEVZATI E,DANURA H,et al.The relationship between IL-6,ET-1 and cerebral vasospasm,in experimental rabbit subarachnoid hemorrhage[J].J Neurosurg Sci,2016 Oct 19.
[58] PENN D L,WITTE S R,KOMOTAR R J,et al.Pathological mechanisms underlying aneurysmal subarachnoid haemorrhage and vasospasm[J].J Clin Neurosci,2015,22(1):1-5.doi:10.1016/j.jocn.2014.05.0
[59] 吴琼,李晓凤,王大路,等.尼莫地平治疗蛛网膜下腔出血后脑血管痉挛的临床观察[J].中国医药导刊,2017,19(2):155-156.
[60] SCHALLNER N,PANDIT R,THOMAS A J,et al.Microglia regulate blood clearance in subarachnoid hemorrhage by heme oxygenase-1[J].J Clin Invest,2015,125(7):2 609-2 625.
(收稿2017-10-15 修回2018-08-28)
本文责编:夏保军
本文引用信息:曲良卓.蛛网膜下腔出血颅内血管痉挛及炎症的相关标记物探讨[J].中国实用神经疾病杂志,2018,21(19):2165-2170.DOI:10.12083/SYSJ.2018.19.470
Reference information:QU Liangzhuo.Discussion on related markers of intracranial vasospasm and inflammation in subarachnoid hemorrhage[J].Chinese Journal of Practical Nervous Diseases,2018,21(19):2165-2170.DOI:10.12083/SYSJ.2018.19.470