目的 分析急性脑血管病患者介入过程中应用数字减影血管造影(DSA)的效果。方法 选取河南大学附属南石医院接受介入手术治疗的100例急性缺血性脑血管疾病患者,在手术过程中应用DSA,并观察其应用价值。结果 通过DSA检查发现急性缺血性脑血管病患者中,血管异常84例,血管正常16例(16.00%);交通动脉瘤占6.00%,大脑动脉狭窄占54.55%。治疗后患者血管狭窄和闭塞情况好于治疗前,差异有统计学意义(P<0.05)。结论 急性缺血性脑血管病采用DSA检查,能够显著提高急性缺血性脑血管病的检出率得
数字减影血管造影在缺血性脑血管病患者介入治疗中的作用
王相阁
河南大学附属南石医院神经外科,河南 南阳 473065
作者简介:王相阁,Email:172289221@qq.com
【摘要】 目的 分析急性脑血管病患者介入过程中应用数字减影血管造影(DSA)的效果。方法 选取河南大学附属南石医院接受介入手术治疗的100例急性缺血性脑血管疾病患者,在手术过程中应用DSA,并观察其应用价值。结果 通过DSA检查发现急性缺血性脑血管病患者中,血管异常84例,血管正常16例(16.00%);交通动脉瘤占6.00%,大脑动脉狭窄占54.55%。治疗后患者血管狭窄和闭塞情况好于治疗前,差异有统计学意义(P<0.05)。结论 急性缺血性脑血管病采用DSA检查,能够显著提高急性缺血性脑血管病的检出率得到,不良反应率低。
【关键词】 数字减影血管造影;急性缺血性脑血管病;介入治疗;应用价值;检出率
【中图分类号】 R743.3 【文献标识码】 A 【文章编号】 1673-5110(2018)21-2394-05 DOI:10.12083/SYSJ.2018.21.512
The value of digital subtraction angiography in the interventional treatment of patients with ischemic cerebrovascular disease
WANG Xiangge
Department of Neurosurgery,Affiliated Hospital of Henan University,Nanyang 473065,China
【Abstract】 Objective To analyze the effect of digital subtraction angiography (DSA) in patients with acute cerebrovascular disease.Methods One hundred patients with acute ischemic cerebrovascular disease who underwent interventional surgery at Nanshi Hospital affiliated to Henan University were enrolled.DSA was applied during the operation and its application value was observed.Results Through DSA examination,84 patients with acute ischemic cerebrovascular disease were found to have vascular abnormalities,16 normal vessels (16.00%),6.00% for traffic aneurysms,and 54.55% for cerebral artery stenosis.The stenosis and occlusion of the patients after treatment were better than before treatment,and the difference was statistically significant (P<0.05).Conclusion DSA examination of acute ischemic cerebrovascular disease can significantly improve the detection rate of acute ischemic cerebrovascular disease,and the adverse reaction rate is low.
【Key words】 Digital subtraction angiography;Acute ischemic cerebrovascular disease;Interventional therapy;Application value;Detection rate
脑血管疾病大多数发病突然[1],如果不及时救治,会导致死亡,给患者的家庭和健康带来极大伤害,已成为社会共同关注的问题之一[2]。急性缺血性脑血管的患者会出现突发神经功能障碍,少数患者伴有突发的意识障碍等情况[3]。对缺血性脑血管病过去主要靠药物治疗,效果往往不够理想[4]。随着医疗技术的飞速发展和新型材料的应用,近年来研究发现,DSA这种新型技术受到了广大群众的认可,可明显提高了脑血管疾病诊断率,改善临床症状有较好疗效[5]。本文选取河南大学附属南石医院神经外科部分脑血管患者为研究对象,分析急性脑血管病患者介入过程中应用数字减影血管造影(DSA)的效果。
1 资料与方法
1.1 临床资料 研究对象为100例急性缺血性脑血管病于2014-02—2015-08在河南大学附属南石医院神经外科接受治疗的患者。男45例,女55例,年龄26~72(53.1±3.9)岁。患者符合脑血管病诊断标准且均经MRI及CT确诊,排除患有心肝肾脏器官方面的重大疾病和免疫性疾病的患者。
1.2 方法 患者在入院后经医生和仪器检查确诊,在手术治疗中介入DSA检查,如患者为血管狭窄和闭塞采用介入手术进行治疗。具体的DSA检查方法如下:将5F的猪尾导管放入患者的升主动脉内,将对比剂注入猪尾导管内,采集患者的头颅正位脑部图像,速度为6帧/s,直到采集出比较清楚在静脉窦时期的图像,然后选择DSA灌注图像的脑实质期。采集完图像后,行重建三维,得到重建的图像,从不同角度仔细观察血管狭窄情况。采用直径为10 mm的正圆形钢球测量患者的血管狭窄情况,依据患者的病变情况及图像种类调节钢球位置。
1.3 观察指标[6] (1)分析在DSA检查中100例急性缺血性脑血管病患者的类型及比例。(2)比较血管狭窄和闭塞患者在治疗前后血管狭窄程度的改变(主要包括血管面积的狭窄程度、血管直径狭窄程度、病变的长度及最小直径等)。
1.4 统计学处理 运用SPSS 17.0软件进行数据处理,计量资料以均数±标准差(x±s)表示,采用t检验,计数资料以率(%)表示,采用卡方检验,P<0.05为差异有统计学意义。
2 结果
2.1 DSA检查中急性缺血性脑血管疾病中的类型及比例 16例患者血管正常(16.00%),血管异常84例(脑动静脉畸形15例,脑动静脉畸形6例,大脑动脉狭窄54例,大脑动脉闭塞9例),大脑动脉狭窄占54.00%,交通动脉瘤占6.00%。
2.2 血管狭窄和闭塞患者治疗前后血管狭窄程度比较 治疗后患者血管狭窄和闭塞情况好于治疗前,差异具有统计学意义(P<0.05)。见表1、图1~5。
表1 患者治疗前后血管狭窄程度比较 (x±s)
Table 1 Comparison of vascular stenosis before and after treatment (x±s)
| 时间 |
n |
面积狭窄程度(%) |
直径狭窄程度(%) |
病变的长度(mm) |
最小直径(mm) |
| 治疗前 |
50 |
47.4±12.7 |
43.6±10.5 |
7.9±2.3 |
0.7±0.2 |
| 治疗后 |
50 |
15.4±4.9 |
13.8±4.4 |
12.3±2.7 |
3.1±0.2 |
| t值 |
|
16.128 0 |
14.875 8 |
7.513 0 |
35.699 6 |
| P值 |
|
<0.05 |
<0.05 |
<0.05 |
<0.05 |
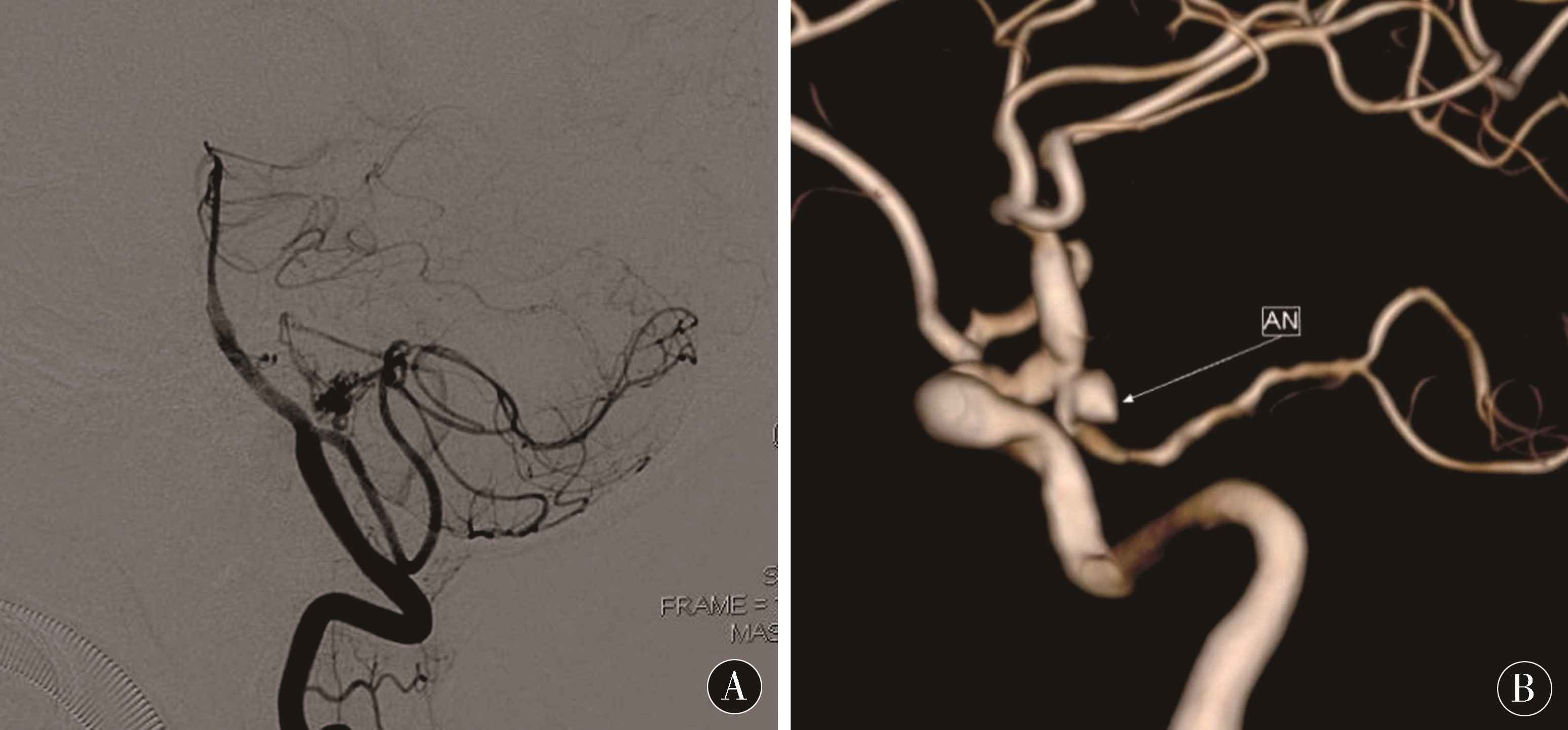
图1 主要由小脑后下动脉供血的动静脉畸形 图2 后交通动脉瘤3D图片
Figure 1 Arteriovenous malformation mainly from the posterior inferior cerebellar artery Figure 2 Post-traffic aneurysm 3D picture
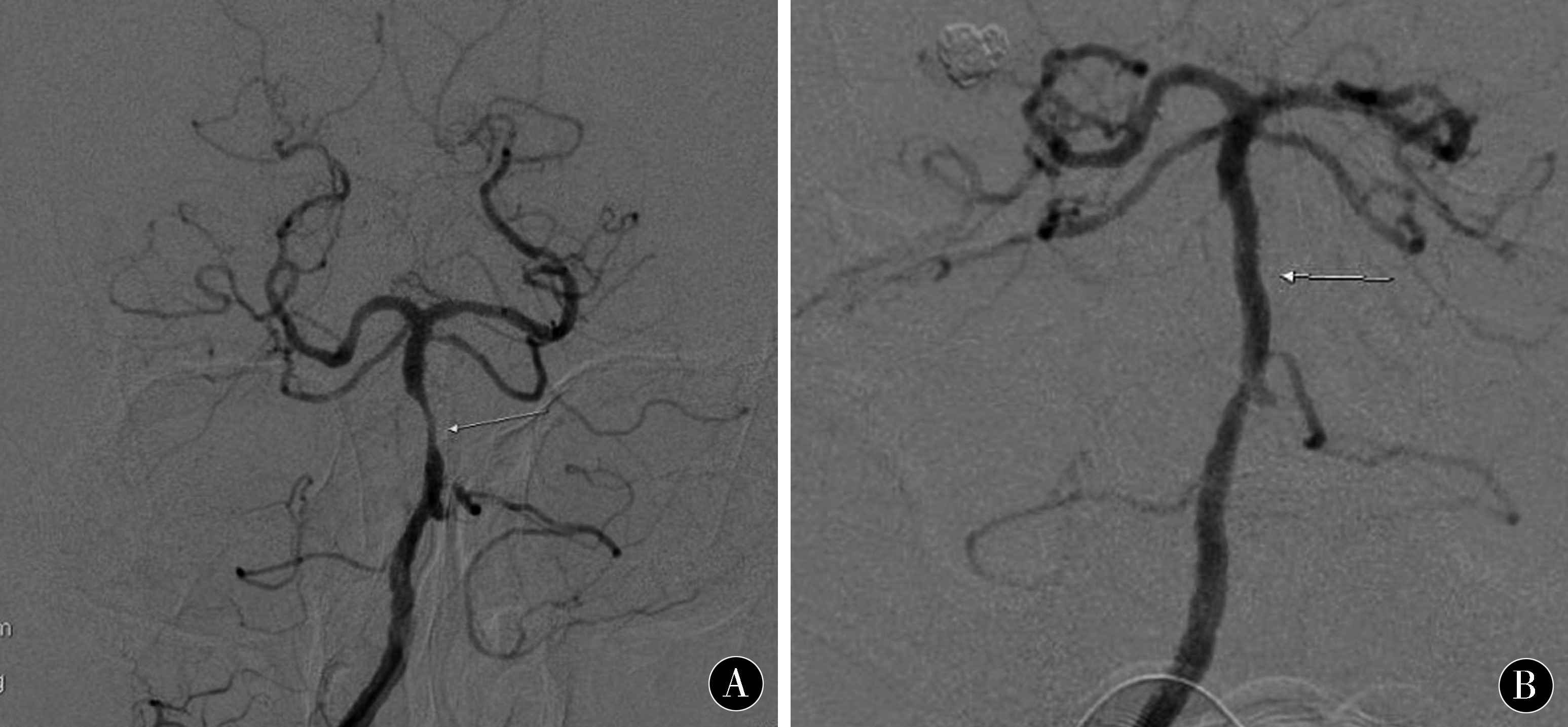
图3 颈内动脉起始段重度狭窄术前后比较
Figure 3 Comparison of severe stenosis of the initial carotid artery
图4 颈内动脉岩骨段重复狭窄术前后比较
Figure 4 Comparison of repeated stenosis of the internal carotid artery
图5 基底动脉近段重度狭窄术前后比较
Figure 5 Comparison of proximal and proximal severe stenosis of basilar artery
3 讨论
随着我国人口老龄化的日益增多,脑血管的发病率增加,且大多发病突然[7-8],给患者健康带来极大的伤害,已经成为社会共同关注的问题之一[9-10]。缺血性脑血管病的主要病症通常有头痛、意识模糊及偏瘫、失语[11-12]。缺血性脑血管病介入治疗的常见并发症有血压下降、高灌注综合征、缺血性卒中、动脉夹层形成、心肌缺血、血管痉挛、颅内出血等[13-14]。缺血性脑血管病出现后卒中或其他血管疾病的发生率明显增多。根据调查发现,缺血性脑血管病出现后2 d内有50%的患者出现脑卒中,5 a有1/3的患者脑组织内有大面积的阻塞[15-16]。以往主要靠药物治疗,但传统的药物很难治愈,效果不理想,所以快速正确的诊断对缺血性脑血病的及时治疗至关重要[17-18]。近年来研究发现,采用DSA介入手术治疗对重新建立缺血部位的血液循环,快速对病情做出有效的判断,为患者在最佳时期进行有效的介入治疗,改善临床症状有较好疗效。目前认为是诊断血管狭窄与闭塞的金标准[19-20]。本文发现,通过DSA检查发现血管异常患者84例,血管正常16例,交通动脉瘤占6.00%,大脑动脉狭窄占54.55%。在血管面积的狭窄程度、血管直径狭窄程度、病变的长度和最小直径方面,治疗后患者情况好于治疗前,差异有统计学意义(P<0.05)。经DSA检查治疗后,再进行手术治疗后取得良好的治疗效果,并发症发生率明显下降,表明通过DSA检查下,介入手术治疗过程应用DSA疗效显著。具体原因:(1)目前,急性缺血性脑血管病的检查方法较多,具体包括造影、超声、CT及DSA等。因受到仪器设备的精准度、仪器使用人员的操作技能等的影响,检查结果都会有些误差,从而影响医生的判断[21-23]。(2)外界因素不会DSA的检查,脑部血管中注入对比剂,根据人类脑部血管的流动性,DSA检查可收集到各个时期的脑部图像,根据收集的图像就可以辨别出发病的位置和病情进展程度,就可以对患者的病情做出判断和制定治疗方案[24-25]。(3)采用DSA辅助介入治疗脑血管疾病,可以将患者脑部血管情况清晰地呈现出来,进而可以快速发现病变位置,从而有效判断病情,提高了治疗的速度,为患者治疗节省了宝贵的时间。与KIDWELL等[26]的研究结论相似。
采用DSA对缺血性脑血管病患者进行诊断,取得良好的治疗效果,患者血管的狭窄程度改善,提升了患者的满意度[27-30]。
4 参考文献
[1] KILBURG C,SCOTT MCNALLY J,DE HAVENON A,et al.Advanced imaging in acute ischemic stroke[J].Neurosurg Focus,2017,42(4):E10.doi:10.3171/2017.1.FOCUS16503.
[2] BARON J C.Recent advances in mesoscopic-scale imag-ing in animal models of ischemic stroke[J].Curr Opin Neurol,2016,29(1):104-111.doi:10.1097/WCO.0000000000000275.
[3] TANSY AP,LIEBESKIND DS.Imaging Acute Ischemic Stroke:Mapping Present and Future Clinical Practice[J].Curr Atheroscler Rep,2015,17(9):50.doi:10.1007/s11883-015-0531-8.
[4] HOLMSTEDT C A,TURAN T N,CHIMOWITZ M I.Atherosclerotic intracranial arterial stenosis:risk factors,diagnosis,and treatment[J].Lancet Neurol,2013,12(11):1 106-1 114.
[5] JAUCH E C,SAVER J L,ADAMS H P Jr,et al Guidelines for the early management of patients with acute ischemic stroke:a guideline for healthcare professionals from the American heart association /American stroke association[J].Stroke,2013,44(3):870-947.
[6] POWERS W J.Cerebral hemodynamics in ischemic cerebrovascular disease[J].Ann Neurol,1991,29(3):231-240.
[7] SZABO K,KERN R,HENNERICI M G.Recent advanc-es in imaging in management of symptomatic internal carotid artery disease[J].Int J Stroke,2007,2(2):97-103.doi:10.1111/j.1747-4949.2007.00103.x.
[8] CHIMOWITZ M I,LYNN M J,DERDEYN C P,et al.Stenting versus aggressive medical therapy for intracra-nial arterial stenosis[J].N Engl J Med,2011,365(11):993-1 003.
[9] DUMONT T M,WACH M M,MOKIN M,et al.Perioperative complications after carotid artery stenting:a contemporary experience from the university at buffalo neuroendovascular surgery team[J].Neurosurgery,2013,73 (4):689-694.
[10] KIDWELL C S,JAHAN R,GORNBEIN J,et al.A trial of imaging selection and endovascular treatment for ischemic stroke[J].N Engl J Med,2013,368(10):914-923.
[11] RAHMAN I,PATEL P,BOGER P,et al.Therapeutic upper gas-trointestinal tract endoscopy in Paediatric Gastroenterolo-gy[J].World J Gastrointest Endosc,2015,7(3):169.
[12] 王彦阔.介入手术与单纯药物干预对缺血性脑血管病患者远期生活质量的改善作用[J].中国实用神经疾病杂志,2017,20(11):74-76.
[13] UEDA T,YUH W T,TAOKA T.Clinical application of perfusion and diffusion MR imaging in acute ischemic stroke[J].J Magn Reson Imaging,1999,10(3):305-309.
[14] ASADI H,DOWLING R,YAN B,et al.Advances in endovascular treatment of acute ischaemic stroke[J].Intern Med J,2015,45(8):798-805.doi:10.1111/imj.12652.Review.
[15] Chen Bin,Jinlin,Zhang Dongzi,et al.Analysis of the efficacy and prognosis of intracranial vascular interventional therapy for ischemic cerebrovascular disease [J].modern biomedicine progress,2017,16 (06):1 131-1 134.
[16] XIN L,HAIYAN L.Progress in clinical research of interventional therapy for ischemic cerebrovascular disea-se [J].Chinese community doctor,2017,10 (09):6-7.
[17] HSIA A W,TONG D C.New magnetic resonance imaging and computed tomography techniques for imaging of acute stroke[J].Curr Atheroscler Rep,2003,5(4):252-259.
[18] FUSTER V.Advances in the diagnosis of arterial disease by magnetic resonance imaging[J].Rev Esp Cardiol,2001,54 Suppl 1:2-7.
[19] CHENGSHI C,LIJUN H.Analysis of the clinical effect of carotid artery stenting in patients with ischemic cerebrovascular disease [J].Chinese medical Frontier Journal:electronic version,2014,6 (3):58-61.
[20] LIU WANTING,XU ZHIQIANG,GUAN HAITAO,et al.Retrospective analysis of interventional surgery for ischemic cerebrovascular disease[J].Chinese Journal of modern surgery,2014,18 (3):215-218.
[21] LIN C S,SHIH C C,YEH C C,et al.Risk of Stroke and Post-Stroke Adverse Events in Patients with Exacerbations of Chronic Obstructive Pulmonary Disease[J].PLoS One,2017,12(1):e0169429.doi:10.1371/journal.pone.0169429.
[22] CAPLAN L R,THOMAS A J,INOA V.Interventional treatment of brain ischemia related to intracranial cerebrovascular occlusive lesions[J].Curr Opin Neurol,2014,27(1):1-7.doi:10.1097/WCO.0000000000000044.
[23] FRERICHS K,BAKER J,NORBASH A.ntra-arterial stroke thrombolysis and carotid stenting:methods for the treatment of ischemic cerebrovascular disease[J].Semin Roentgenol,2002,37(4):255-265.
[24] LI H,WU Y.Prognosis comparisons in acute ischemic stroke patients with thrombolysis and nonthrombolysis therapy:a retrospective study with larger sample size[J].Blood Coagul Fibrinolysis,2018,29(2):178-183.doi:10.1097/MBC.0000000000000685.
[25] LIU M,PAN Y,ZHOU L,et al.Predictors of post-thrombolysis symptomatic intracranial hemorrhage in Chinese patients with acute ischemic stroke[J].PLoS One,2017,12(9):e0184646.doi:10.1371/journal.pone.0184646.
[26] PAN X,ZHU Y,ZHENG D,et al.Prior antiplatelet agent use and outcomes after intravenous thrombolysis with recombinant tissue plasminogen activator in acute ischemic stroke:a meta-analysis of cohort studies and randomized controlled trials[J].Int J Stroke,2015,10(3):317-323.doi:10.1111/ijs.12431.
[27] MAYBERG M R.Carotid artery stenosis[J].Neuro-surg,2014,99(2):225-227.
[28] DE ABAJO F J,RODRGUEZ-MARTN S,RODRGUEZ-MIGUEL A,et al.Risk of Ischemic Stroke Associated With Calcium Supplements With or Without Vitamin D:A Nested Case-Control Study[J].J Am Heart Assoc,2017,6(5).pii:e005795.doi:10.1161/JAHA.117.005795.
[29] HUAIZHANG S,DOU L,SHENMAO L,et al.The etiological characteristics of 1000 Chinese patients with ischemic cerebrovascular disease by DSA analysis [J].Chinese Journal of cerebrovascular disease,2005,2(10):437-440.
[30] OGATA T,MATSUO R,KIYUNA F,et al.Left Atrial Size and Long-Term Risk of Recurrent Stroke After Acute Ischemic Stroke in Patients With Nonvalvular Atrial Fibrillation[J].J Am Heart Assoc,2017,6(8).pii:e006402.doi:10.1161/JAHA.117.006402.
(收稿2017-02-23 修回2018-08-08)
本文责编:王喜梅
本文引用信息:王相阁.数字减影血管造影在缺血性脑血管病患者介入治疗中的作用[J].中国实用神经疾病杂志,2018,21(21):2394-2398.DOI:10.12083/SYSJ.2018.21.512
Reference information:WANG Xiangge.The value of digital subtraction angiography in the interventional treatment of patients with ischemic cerebrovascular disease[J].Chinese Journal of Practical Nervous Diseases,2018,21(21):2394-2398.DOI:10.12083/SYSJ.2018.21.512