目的 观察维生素B12(vitamin B12,VitB12)、叶酸(folic acid,FA)、同型半胱氨酸(homocysteine,Hcy)在帕金森异动症患者血浆中的变化,分析VitB12水平变化的相关因素。方法 237例帕金森病患者根据异动症定义分为异动症组(63例)和非异动症组(174例),比较2组血浆VitB12、FA、Hcy水平,将差异有统计学意义的指标选出,异动症组按性别、年龄、起病年龄、病程、左旋多巴使用时间、日多巴总量、H-Y分期分组,并进行组间对比。结果 异动症组血浆Hcy、
帕金森病合并异动症患者血浆维生素B12水平的相关因素研究
王 丽 王小平 李庭毅△
孝感市中心医院神经内科,湖北 孝感 432000
作者简介:王丽,主治医师,Email:lryz2014@163.com
△通信作者:李庭毅,主任医师,Email:ltypsh2014@163.com
【摘要】 目的 观察维生素B12(vitamin B12,VitB12)、叶酸(folic acid,FA)、同型半胱氨酸(homocysteine,Hcy)在帕金森异动症患者血浆中的变化,分析VitB12水平变化的相关因素。方法 237例帕金森病患者根据异动症定义分为异动症组(63例)和非异动症组(174例),比较2组血浆VitB12、FA、Hcy水平,将差异有统计学意义的指标选出,异动症组按性别、年龄、起病年龄、病程、左旋多巴使用时间、日多巴总量、H-Y分期分组,并进行组间对比。结果 异动症组血浆Hcy、FA水平与非异动症组比较差异无统计学意义(P>0.05)。异动症组血浆VitB12水平与非异动症组比较差异有统计学意义(P<0.01)。异动症组中不同性别、年龄、起病年龄、病程、使用多巴时间及H-Y分期患者血浆维生素B12水平无明显差异(P>0.05),而不同日多巴总量患者血浆VitB12水平差异有统计学意义(P<0.05),且日多巴总量越大,血浆VitB12水平越低。结论 帕金森病异动症患者血浆VitB12水平明显降低,影响异动症患者血浆VitB12变化的因素为日多巴总量。
【关键词】 帕金森病;异动症;维生素B12;叶酸;同型半胱氨酸;左旋多巴
【中图分类号】 R742.5 【文献标识码】 A 【文章编号】 1673-5110(2018)09-0961-04 DOI:10.12083/SYSJ.2018.09.241
Related factor study on plasma vitamin B12 in patients with Parkinson’s disease and dyskinesias
WANG Li,WANG Xiaoping,LI Tingyi
Department of Neurology,Central Hospital of Xiaogan,Xiaogan 432000,China
【Abstract】 Objective To observe the changes of plasma levels of vitamin B12,folic acid,homocysteine and the relevant factor of causing change in patients with Parkinson’s disease and dyskinesias.Methods 237 patients of Parkinson’s disease were divided into dyskinesias (63 patients) and non-dyskinesias (174 patients) according to the clinical definition of dyskinesias.Plasma levels of vitamin B12,folic acid,homocysteine in two groups were compared.Then,we elected discrepant indicator and contrasted its difference in the different gender,age,age onset,duration,the cumulative time of medication of levodopa,daily volume dose of levodopa and Hoehn-Yahr staging in dyskinesias.Results The difference of the plasma levels of Hcy and FA of dyskinesias and non-dyskinesias wasn’t statistical significance (P>0.05).The difference of the plasma level of vitamin B12 of dyskinesias and non-dyskinesias was statistical significance (P<0.01).The plasma level of vitamin B12of dyskinesias weren’t statistically significant difference in terms of gender,age,age onset,duration,the cumulative time of medication of levodopa,and Hoehn-Yahr staging (P>0.05).The plasma level of vitamin B12 of dyskinesias related to the daily volume dose of levodopa was statistical significance (P<0.05).The bigger daily volume dose of levodopa,the lower plasma level of vitamin B12.Conclusion The plasma level of vitamin B12 of dyskinesias is lower.The factor affecting the plasma level of vitamin B12 of dyskinesiasis the daily volume dose of levodopa.
【Key words】 Parkinson’s disease;Dyskinesias;Vitamin B12;Folic acid;Homocysteine;Levodopa
帕金森病(Parkinson’s disease,PD)是一种神经系统变性疾病[1]。目前主要用药仍是左旋多巴,随着治疗时间及病程的延长,发生异动症的概率随之增加,超过10 a发生异动症概率高达80%[2-4]。VitB12、FA在帕金森病患者中降低而Hcy升高已被证实[5-8],但VitB12、FA、Hcy在帕金森病异动症患者中的变化目前国内还未见报道。本研究对比了帕金森病异动症与非异动症患者VitB12、FA、Hcy水平,分析其可能影响因素。
1 资料与方法
1.1 研究对象 收集孝感市中心医院2015-01—2016-11 PD门诊及住院患者237例。(1)入选标准:符合英国脑库制定的原发性PD诊断标准:①必须存在至少下列两项主征:静止性震颤、运动迟缓、肌强直及步态姿势异常;②排除药物、脑血管病、脑炎及脑外伤等各种原因导致的帕金森综合征和进行性核上性眼肌麻痹、橄榄-脑桥-小脑萎缩、黑质-纹状体变性等帕金森叠加综合征;③左旋多巴治疗有效;④初发症状、体征或病程中有两侧不对称。(2)排除标准:脑卒中、脑肿瘤、脑炎、脑积水、脑外伤及先天性VitB12、FA、Hcy缺乏或不足者。
1.2 方法 根据异动症临床定义[9]将237例PD患者分为异动症组63例和非异动症组174例。入组次日清晨采用肝素抗凝管抽取肘静脉血3 mL,1 h内分离血浆,置于—20 ℃冰箱内待查,采用放射免疫法检测VitB12、FA水平,采用酶分析法检测Hcy水平。
观察2组血浆VitB12、FA、Hcy水平;将差异有统计学意义的指标选出,异动症组按性别、年龄、起病年龄、病程、左旋多巴使用时间、日多巴总量、H-Y分期的不同分组进行选出指标的对比。
1.3 统计学分析 采用SPSS 22.0统计软件进行数据分析,计量资料采用均数±标准差(x±s)表示,2组比较采用独立样本t检验,多组比较采用单因素方差分析。P<0.05为差异有统计学意义。
2 结果
2.1 2组血浆FA、Hcy VitB12水平比较 异动症组血浆Hcy、FA水平与非异动症组比较差异无统计学意义(分别为t=0.909,P>0.05;t=0.407,P>0.05)。异动症组血浆VitB12水平与非异动症组比较差异有统计学意义(t=-3.486,P<0.01)。见表1。
表1 2组血浆VitB12、FA、Hcy水平比较 (x±s)
| 组别 |
n |
VitB12(ng/mL) |
FA (pg/mL) |
Hcy(μmol/L) |
| 异动症组 |
63 |
312.47±163.22 |
9.13±4.21 |
19.65±11.60 |
| 非异动症组 |
174 |
410.46±200.26 |
8.87±4.48 |
18.33±9.20 |
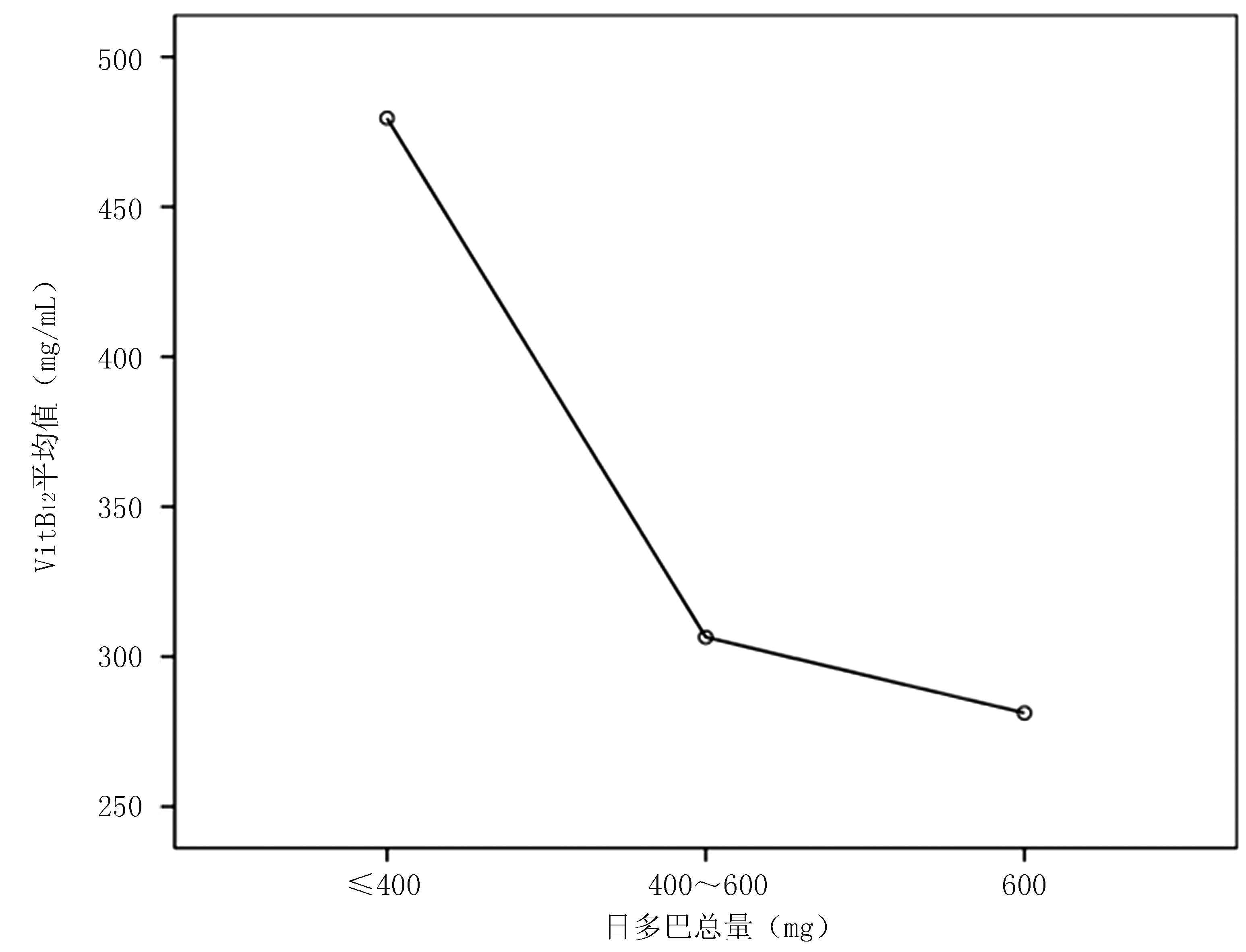
2.2 影响异动症血浆VitB12变化的因素分析 不同性别、年龄、起病年龄、病程、左旋多巴使用时间、H-Y分期患者的血浆VitB12差异均无统计学意义(P>0.05)。日多巴总量分为<400 mg、400~600 mg、>600 mg 3组,日多巴总量<400 mg组与400~600 mg组及>600 mg组血浆VitB12水平差异有统计学意义(P<0.05),而日多巴总量400~600 mg组与>600 mg组血浆VitB12水平差异无统计学意义(P>0.05)。见表2~4、图1。
图1 日多巴总量与血浆VitB12水平的关系
表2 异动症组不同H-Y分期患者血浆VitB12比较 (x±s)
| H-Y分期 |
n |
VitB12(ng/mL) |
| Ⅰ~Ⅱ期 |
15 |
315.14±196.25 |
| Ⅲ期 |
28 |
277.34±110.81 |
| Ⅳ~Ⅴ期 |
20 |
359.63±192.19 |
表3 异动症组不同日多巴总量患者血浆VitB12比较 (x±s)
| 日多巴总量 |
n |
VitB12(ng/mL) |
| <400 mg |
7 |
479.57±263.70 |
| 400~600 mg |
23 |
306.49±93.82 |
| >600 mg |
33 |
281.18±159.31 |
表4 帕金森病异动症组不同指标患者血浆VitB12水平比较 (x±s)
| 指标 |
|
n |
VitB12(ng/mL) |
P值 |
| 性别 |
男 |
33 |
313.76±185.10 |
>0.05 |
| 女 |
30 |
311.04±138.36 |
| 年龄 |
≤60岁 |
13 |
249.26±112.73 |
>0.05 |
| >60岁 |
50 |
328.90±171.05 |
| 起病年龄 |
≤50岁 |
13 |
263.64±113.54 |
>0.05 |
| >50岁 |
50 |
325.16±172.49 |
| 病程 |
≤5 a |
3 |
300.45±200.60 |
>0.05 |
| >5 a |
60 |
313.07±163.16 |
| 多巴使用时间 |
≤5 a |
5 |
359.57±177.50 |
>0.05 |
| >5 a |
58 |
304.40±162.95 |
3 讨论
PD是一种中老年人常见的神经系统退行性疾病,50岁以上发病率为2%,发病机制为多巴胺神经元变性坏死,多巴胺神经递质合成减少,纹状体多巴胺与乙酰胆碱比例失调[9-12]。随着左旋多巴治疗PD时间的延长,发生异动症的概率随之增加,左旋多巴治疗5 a内异动症的发生率11%,6~9 a发生率32%,>10 a合并异动症者可高达80%[2,13-14]。多数文献报道[5-7,15-18],PD患者Hcy升高、FA及VitB12 降低,且Hcy与FA、VitB12呈负相关。MADENCI等[19]研究发现,PD患者血浆VitB12水平与H-Y分期呈负相关。但异动症组与非异动症组中Hcy、FA及VitB12是否有差异未完全知晓。KOCER等研究[5]表明,Hcy与帕金森异动症无关。而CAMICIOLI等研究[6]表明,高VitB12可能有更低的异动症风险。
本研究中,异动症与非异动症患者血浆FA、Hcy水平无明显差异(P>0.05),而血浆VitB12水平差异有统计学意义,异动症组血浆VitB12水平远低于非异动症组,与CAMICIOLI 等[6]的研究相符。异动症组中不同性别、年龄、起病年龄、病程、左旋多巴使用时间、H-Y分期患者血浆VitB12水平无显著差异(P>0.05),而日多巴总量<400 mg、400~600 mg、>600 mg组间血浆VitB12水平差异有统计学意义(P<0.05),说明日多巴总量400 mg是本研究帕金森病伴异动症患者血浆VitB12水平的一个分界值,日多巴总量>400 mg者比<400 mg者血浆VitB12水平更低。根据日多巴总量与血浆VitB12水平图亦可看出,日多巴总量越大,VitB12水平越低。多数研究[2,20-23]中,日多巴总量>400 mg的帕金森病患者异动症的发生率明显增高,可能提示在临床工作中,对于日多巴总量>400 mg的患者,可适量补充VitB12,从而降低异动症发生的风险。
VitB12是唯一含金属的维生素,是细胞合成核苷酸的重要辅酶,参与脱氧核酸合成,脂肪、碳水化合物及蛋白质的代谢[24-25];参与机体甲基的转化及叶酸的代谢,提高叶酸利用率,VitB12与叶酸一起参与蛋氨酸的合成,降低Hcy浓度[26-27];VitB12维护神经髓鞘的代谢与功能,缺乏时可造成进行性或弥漫性神经脱髓鞘,破坏神经细胞的正常形态及功能,降低神经冲动的泛化、减少抽动等,诱发各种神经疾病[28-30]。灵长类动物实验证明,VitB12可调节氧化还原依赖机制、保护神经、增加脑组织对氧化应激的耐受性,VitB12降低能引起脑内神经元退化[31-34]。本研究血浆VitB12水平降低可能与上述一条或几条机制相关,具体机制还有待进一步的研究。
4 参考文献
[1] THENGANATT M A,JANKOVIC J.Parkinson disease subtypes[J].JAMA Neurol,2014,71(4):499-504.
[2] CHONDROGIORGI M,TATSIONI A,REICHMANN H,et al.Dopamine agonist monotherapy in Parkinson’s disease and potential risk factors for dyskinesia:a meta-analysis of levodopa-controlled trials[J].Eur J Neurol,2014,21(3):433-440.
[3] FIORENTINI C,SAVOIA P,SAVOLDI D,et al.Receptor heteromers in Parkinson's disease and L-DOPA-induced dyskinesia[J].CNS Neurol Disord Drug Targets,2013,12(8):1 101-1 113.
[4] HUOT P,JOHNSTON T H,KOPRICH J B,et al.The pharmacology of L-DOPA-induced dyskinesia in Parkinson's disease[J].Pharmacol Rev,2013,65(1):171-222.
[5] KOCER B,GUVEB H,CONKBAYIR I,et al.The Effect of Hyperhomocysteinemia on Motor Symptoms,Cogni-tive Status,and Vascular Risk in Patients with Parkin-son’s Disease[J].Parkinson’s Dis,2016,8(6):1 103-1 115.
[6] CAMICIOLI R M,BOUCHARD T P,SOMERVILLE M J.Homocysteine is not associated with global motor or cognitive measuers in nondemented older Parkinson’s disease patients[J].Mov Disord,2009,24(2):176-182.
[7] MILLER J W,SELHUB J,NADEAU M R,et al.Effect of L-dopa on plasma homocysteinein PD patients relationship to B-vitamin status[J].Neurology,2003,60(7):1 125-1 129.
[8] BENKLER M,AGMON-LEVIN N,HASSIN-BAER S,et al.Immunology,autoimmunity,and autoantibodies in Parkinson's diseasee[J].Clin Rev Allergy Immunol,2012,42(2):164-171.
[9] GURIDI J,GONZALEZ-REDONDO R,OBESO J A.Clinical features,pathophysiology,and treatment of levopa-induced dyskinesias in Parkinson’s disease[J].Parkinsons Dis,2012:9431599.
[10] DHALL R,KREITZMAN D L.Advanced in levodopa therapy for Parkinson disease:Review of RYTARY (carbidopa and levodopa)clinical efficacy and safety[J].Neurology,2016,86(14):S13-S24.
[11] RIECK M,SCHUMACHER-SCHUH A F,ALTMANN V,et al.DRD2 haplotype is associated with dyskinesia induced by levodopa therapy in Parkinson's disease patients[J].Pharmacogenomics,2012,13(15):1 701-1 710.
[12] KO W K,LI Q,BEZARD E.Effects of L-tryptophan on L-DOPA-induced dyskinesia in the L-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)-treated macaque model of Parkinson's disease[J].Neurosci Lett,2014,566:72-76.
[13] ALEGRE M,LPEZ-AZCRATE J,ALONSO-FRECH F,et al.Subthalamic activity during diphasic dyskinesias in Parkinson's disease[J].Mov Disord,2012,27(9):1 178-1 181.
[14] DOTCHIN C L,GRAY W K,DEWHURST F,et al.Parkinson's disease related dyskinesia in a Tanzanian population[J].Parkinsonism Relat Disord,2015,21(9):1 109-1 110.
[15] MEMEDI M,WESTIN J,NYHOLM D.Spiral drawing during self-rated dyskinesia is more impaired than during self-rated Off[J].Parkinsonism Relat Disord,2013,19(5):553-556.
[16] FRANCARDO V,CENCI M A.Investigating the molecular mechanisms of L-DOPA-induced dyskinesia in the mouse[J].Parkinsonism Relat Disord,2014,20(Suppl 1):S20-S22.
[17] IRAVANI M M,MCCREARY A C,JENNER P.Striatal plasticity in Parkinson's disease and L-dopa induced dyskinesia[J].Parkinsonism Relat Disord,2012,18(Suppl 1):S123-S125.
[18] GRIFFITHS R I,KOTSCHET K,ARFON S,et al.Automated assessment of bradykinesia and dyskinesia in Parkinson's disease[J].J Parkinsons Dis,2012,2(1):47-55.
[19] MADENCI G,BILEN S,ARLI B,et al.serum iron,Vitamin B12 and folic acid levels in parkinson’s disease[J].Neurochem Res,2012,37(7):1 436-1 441.
[20] JENNER P.Wearing off,dyskinesia,and the use of continuous drug delivery in Parkinson's disease[J].Neurol Clin,2013,31(3 Suppl):S17-S35.
[21] GORGONE G,CURRO M,FERLAZZO N,et al.Coenzyme Q10,hyperhomocysteinemia and MTIIFR C677T polymorphism in levodopa-treated Parkinson’s disease patients[J].Neuromolecular Med,2012,14(1):84-90.
[22] MICHALOWSKA M,FISZER U,SZATANOWSKI T.Motor levodopa-induced complication in Parkinson’s disease[J].Pol Merkur Lekarski,2016,40(240):357-361.
[23] POLITIS M,OERTEL W H,WU K,et al.Graft-induced dyskinesias in Parkinson's disease: High striatal serotonin/dopamine transporter ratio[J].Mov Disord,2011,26(11):1 997-2 003.
[24] KADOWAKI T,KOMAGAMINE T,SUZUKI K,et al.Oseltamivir-induced dyskinesia in Parkinson's disease[J].Parkinsonism Relat Disord,2011,17(2):133-134.
[25] BARKER R A,KUAN W L.Graft-induced dyskinesias in Parkinson's disease: what is it all about?[J].Cell Stem Cell,2010,7(2):148-149.
[26] STATHIS P,KONITSIOTIS S,ANTONINI A.Dopamine agonists early monotherapy for the delay of development of levodopa-induced dyskinesias[J].Expert Rev Neurother,2015,15(2):207-213.
[27] CERVANTES-ARRIAGA A,RODRGUEZ-VIOLANTE M,GONZLEZ-LATAP P,et al.ApoE polymorphisms and dopaminergic replacement therapy in Parkinson's disease[J].Rev Med Inst Mex Seguro Soc,2014,52(1):14-18.
[28] LIASHCHENKO E A,SKRIPKINA N A,LEVIN O S.Influence of levodopa,stalevo on dyskinesia in Parkinson's disease:STRIDE-PD study[J].Zh Nevrol Psikhiatr Im S S Korsakova,2013,113(7 Pt 2):62-68.
[29] KHAN T S.Off spells and dyskinesias: pharmacologic management of motor complications[J].Cleve Clin J Med,2012,79(Suppl 2):S8-S13.
[30] SAM A,PREZ-LOPEZ C,ROMAGOSA J,et al.Dyskinesia and motor state detection in Parkinson's disease patients with a single movement sensor[J].Conf Proc IEEE Eng Med Biol Soc,2012,2012:1 194-1 197.
[31] RAJABALLY Y A,MARTEY J.Levodopa,Vitamins,ageing and the neuropathy of Parkinson’s disease[J].J Neurol,2013,260(11):2 844-2 848.
[32] MCCADDON A.Vitamin B12 in neurology and ageing:Clinical and genetic aspects[J].Biochimie,2013,95(5):1 066-1 076.
[33] SHEN L.Association beweeten B Vitamins and Parkinson’s disease[J].Nutrients,2015,7(9):7 190-9 208.
[34] HEUMANN R,MORATALLA R,HERRERO M T,et al.Dyskinesia in Parkinson's disease:mechanisms and current non-pharmacological interventions[J].J Neurochem,2014,130(4):472-489.
(收稿2018-03-17 修回2018-03-27)
本文编辑:夏保军
本文引用信息:王丽,王小平,李庭毅.帕金森病合并异动症患者血浆维生素B12水平的相关因素研究[J].中国实用神经疾病杂志,2018,21(9):961-965.DOI:10.12083/SYSJ.2018.09.241