目的 观察认知康复训练结合头皮针治疗脑卒中后认知功能障碍的疗效。方法 将郑州人民医院康复医学科收治的120例脑卒中后认知功能障碍的患者随机分为头皮针治疗组、认知康复训练组、头皮针治疗联合认知康复训练组(联合治疗组)和对照组各30例,均给予神经内科常规药物治疗,头皮针治疗组、认知训练组、联合组分别给予头皮针治疗、认知康复训练、头皮针治疗结合认知康复训练,对照组除常规神经内科给药外不进行其他系统训练或药物治疗。治疗前及治疗后1个月、3个月、6个月分别用蒙特利尔认知估量表(MoCA)进行评定。结果 治疗后3个月及6个月3组相对于对照组的MoCA评分均有升高,差异有统计学意义(P<0.05);与治疗后3个月相比,治疗后6个月MoCA评分无显著提升(P>0.05)。治疗后3个月及6个月,联合治疗组MoCA评分相对于单纯头皮针治疗组和单纯认知康复训练组明显升高,差异有统计学意义(P<0.05)。相对于对照组,治疗后3个月3组韦氏评分均有显著提升(P<0.05)。结论 认知康复训练结合头皮针治疗可明显改善脑卒中后认知障碍患者的认知功能。
认知康复训练结合头皮针治疗脑卒中后认知功能障碍的疗效观察
车文生 蔡 琛△
郑州人民医院康复医学科,河南郑州 450003
基金项目:河南省科技攻关项目(编号:182102310537)
作者简介:车文生,Email:henwensheng0321@outlook.com
△通信作者:蔡琛,Email:gdgn222@126.com
【摘要】 目的 观察认知康复训练结合头皮针治疗脑卒中后认知功能障碍的疗效。方法 将郑州人民医院康复医学科收治的120例脑卒中后认知功能障碍的患者随机分为头皮针治疗组、认知康复训练组、头皮针治疗联合认知康复训练组(联合治疗组)和对照组各30例,均给予神经内科常规药物治疗,头皮针治疗组、认知训练组、联合组分别给予头皮针治疗、认知康复训练、头皮针治疗结合认知康复训练,对照组除常规神经内科给药外不进行其他系统训练或药物治疗。治疗前及治疗后1个月、3个月、6个月分别用蒙特利尔认知估量表(MoCA)进行评定。结果 治疗后3个月及6个月3组相对于对照组的MoCA评分均有升高,差异有统计学意义(P<0.05);与治疗后3个月相比,治疗后6个月MoCA评分无显著提升(P>0.05)。治疗后3个月及6个月,联合治疗组MoCA评分相对于单纯头皮针治疗组和单纯认知康复训练组明显升高,差异有统计学意义(P<0.05)。相对于对照组,治疗后3个月3组韦氏评分均有显著提升(P<0.05)。结论 认知康复训练结合头皮针治疗可明显改善脑卒中后认知障碍患者的认知功能。
【关键词】 脑卒中;脑血管病;认知功能障碍;认知康复训练;头皮针
【中图分类号】 R743.3 【文献标识码】 A 【文章编号】 1673-5110(2018)24-2719-06 DOI:10.12083/SYSJ.2018.24.567
Effect of cognitive rehabilitation training combined with scalp acupuncture on cognitive dysfunction after stroke
CHE Wensheng,CAI Chen
Department of Rehabilitation Medicine,the People's Hospital of Zhengzhou,Zhengzhou 450003,China
【Abstract】 Objective To observe the effect of cognitive rehabilitation training combined with scalp acupuncture on cognitive dysfunction after stroke.Methods 120 patients with cognitive impairment after stroke admitted in Zhengzhou people's Hospital were randomly divided into the scalp needle therapy group,the cognitive rehabilitation training group,the scalp needle therapy combined with cognitive rehabilitation training group (joint treatment group) and the control group,each group with 30 patients.The cognitive training group and the joint group were given scalp needle therapy,cognitive rehabilitation training,scalp needle therapy combined with cognitive rehabilitation training.The control group did not carry out other systematic training or drug treatment in addition to the conventional neurology medicine.The Montreal cognitive assessment scale (MoCA) was used before and 1 months,3 months and 6 months after treatment respectively.Results The MoCA scores of the three groups were significantly higher than those of the control group at 3 months and 6 months after treatment (P<0.05),but there was no significant improvement in MoCA scores at 6 months after treatment (P>0.05).At the same time,the MoCA score of the combined treatment group was significantly higher than that of the scalp acupuncture group and the cognitive rehabilitation training group at 3 months and 6 months after treatment (P<0.05).In addition,compared with the control group,the Wechsler scores of the three groups at 3 months after treatment were significantly improved (P<0.05).Conclusion Cognitive rehabilitation training combined with scalp acupuncture can significantly improve the cognitive function of patients with cognitive impairment after stroke.
【Key words】 Stroke;Cerebrovascular disease;Cognitive dysfunction;Cognitive rehabilitation training;Scalp needle
认知功能障碍(post-stroke cognitive impairment,PSCI)是脑卒中患者较常见的后遗症之一,脑血管病患者多数均伴不同程度的认知功能损害[1-2]。有学者报道,国内脑卒中患者发病3个月内认知障碍的发生率高达56.6%[3],主要表现为记忆力障碍、计算力障碍、言语障碍、空间定向能力障碍等[4]。认知功能障碍不但严重影响患者的整体功能康复,同时也给患者家庭带来沉重的经济和精神负担,所以对脑卒中后认知功能障碍进行早期干预,有利于患者整体功能的康复,对减轻患者家庭经济和精神负担、提高患者的生活质量具有重要意义。本研究探讨认知康复训练结合头皮针治疗脑卒中后认知功能障碍的疗效。
1 资料与方法
1.1 一般资料 选取2016-01—2018-01在郑州人民医院康复医学科住院治疗的120例脑卒中患者,男78例,女42例,年龄37~67(54.3±8.1)岁。所有患者经头颅CT或颅脑MRI检查证实处于脑梗死或脑出血恢复期,与2016版《中国脑血管病诊治指南与共识》[5]的相关诊断标准相符。纳入标准:(1)首次发生脑卒中,病程<6个月且存在一定程度的认知功能障碍;(2)卒中前无认知功能障碍,卒中后存在认知功能障碍;(3)教育程度为小学以上;(4)排除存在明显的视觉、听觉、视觉障碍者;(5)排除严重意识障碍、痴呆和精神异常而不能配合治疗;(6)各项生命体征平稳,无严重的心、肝、肾功能不全等。将120例患者随机分为4组各30例,头皮针治疗组男18例,女12例;年龄(53.7±7.3)岁;初中学历17例,高中学历6例,大学学历7例;脑梗死21例,脑出血9例;病程(88.5±9.8)d。认知康复训练组男19例,女11例;年龄(57.4±6.3)岁;初中学历15例,高中学历5例,大学学历10例;脑梗死18例,脑出血12例;病程(91.5±6.3)d。联合治疗组男20例,女10例;年龄(56.6±6.3)岁;初中学历13例,高中学历9例,大学学历8例;脑梗死17例,脑出血13例;病程(71.6±8.3)d。对照组男21例,女9例;年龄(59.3±5.3)岁;初中学历18例,高中学历4例,大学学历8例;脑梗死16例,脑出血14例;病程(78.6±5.9)d。各组间一般资料比较差异无统计学意义(P>0.05)。
1.2 方法
1.2.1 常规药物治疗和常规康复训练:每组均给予神经内科常规药物治疗以对基础疾病进行对症治疗,营养神经以改善脑功能等,同时进行简单的常规康复训练,包括含肢体姿势的摆放、异常姿势的控制、体位的变换转移、站立姿势训练、平衡能力训练、四肢功能训练及日常生活功能训练[6]。
1.2.2 认知康复训练方法:根据《Loewenstein认知评定量表》[7],针对认知训练组和联合治疗组患者存在的具体认知功能障碍给予针对性的个体化认知功能训练:①注意力训练:根据患者个体的情况,设计从简单到复杂训练方法,如视觉跟踪、猜测作业、删除作业等,对注意力进行系统的训练。②记忆力训练:通过患者自己和借助他人的帮助、辅助工具的使用等唤醒缺失的部分记忆,同时利用窦祖林教授编制的“记忆训练课程”软件,采用背数、词语配对、短文复述、图片记忆等方法和联想法、编故事法、方位法、分段法等技巧对患者进行记忆力训练[8]。③计算力训练:训练内容先从简单开始然后慢慢增加难度:先让患者计算10以内的加减运算,熟练后再行20以内的加减运算和10以内的乘除法,循序渐进逐渐增加到100以内的加减乘除运算,训练过程中可结合日常生活常用的场景,如市场或超市的购物场景,以免训练过于单调。④思维能力训练:根据患者个体具体情况不同,适当做一些简单的分析、推理训练,如情景推理、图片推理等。⑤空间知觉障碍训练:通过患者自身躯体侧别辨认训练,如使其识记左、右手,进一步认识记忆左手侧为左侧右手外侧为右侧等;然后进行方向训练,通过病房周围的参照物让患者记住东西及南北侧等方位[9]。以上训练每次30 min,1次/d,每周5次,4周为1个疗程,6个疗程共24周。
1.2.3 头皮针治疗方法:头皮针治疗组在常规药物和常规康复训练基础上给予头皮针治疗,不进行系统认知功能训练;联合治疗组除头皮针治疗外,增加系统的认知功能训练。头皮针治疗的具体方法:按照《微针系统诊疗学》的规范,取中额中线、顶中线、病变侧颞前线、病变侧颞后线[10],针刺部位用安尔碘皮肤消毒液常规消毒,选用一次性40 mm钢针常规消毒后进针约30 mm,然后接电针仪,选200次/min连续波型,每次治疗30 min,1次/d,每周5次,4周为1个疗程,治疗6个疗程共24周。
1.3 疗效评定标准
1.3.1 蒙特利尔认知评估量表(MoCA)[11]:包括视空间与执行能力、命名、注意、计算、语言、抽象、回忆、定向等[12],满分30分,对高中以下学历者总分加1分,分数越高代表认知功能越好。
1.3.2 韦氏成人智力量表[13]:①显效:分值达到正常或提高20分以上;②有效:分值提高10~20分;③无效:分值提高<10分或降低。
1.4 统计学处理 采用SPSS 22.0统计学软件对数据进行统计学分析,计量资料以均数±标准差(x±s)表示,组间比较采用t检验。P<0.05为差异有统计学意义。
2 结果
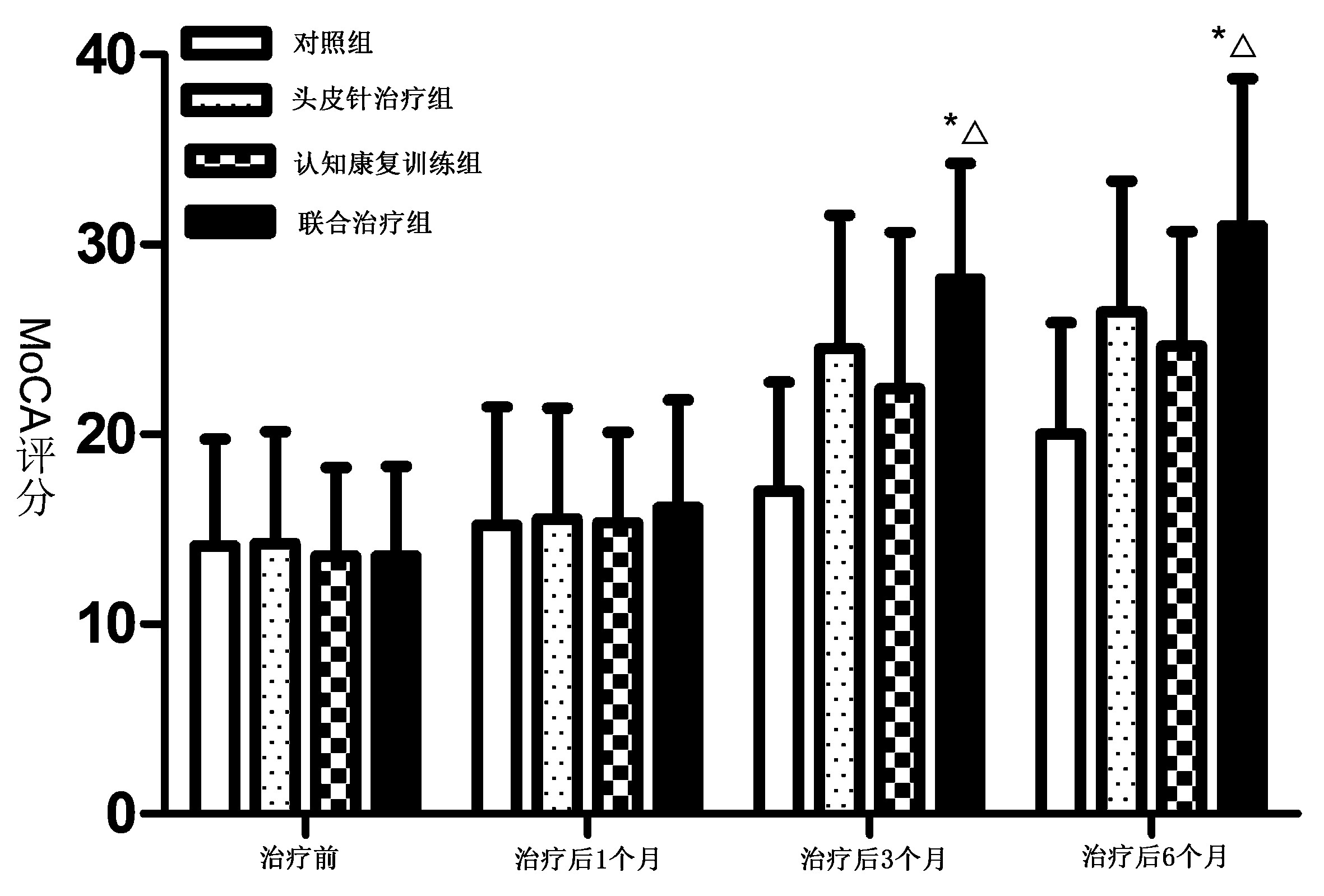
2.1 治疗后各组MoCA评分变化 与治疗前相比,治疗后1个月3组患者相对于对照组的MoCA评分无明显升高(P>0.05);治疗后3个月及6个月3组患者相对于对照组的MoCA评分均有升高,差异有统计学意义(P<0.05);与治疗后3个月相比,治疗后6个月患者的MoCA评分并无显著提升(P>0.05)。治疗后3个月及6个月,联合治疗组MoCA评分相对于单纯头皮针治疗组和单纯认知康复训练组明显升高,差异有统计学意义(P<0.05)。见图1。
2.2 韦氏成人智力力量表评分 相对于对照组,治疗后3个月3组韦氏评分均有显著提升(P<0.05);相对于单纯头皮针治疗组和单纯认知康复训练组,联合治疗组韦氏评分并无显著提升(P>0.05)。见表1。
3 讨论
脑卒中是临床常见的急性脑血管疾病,包括缺血性卒中和出血性卒中[14-15]。随着人们生活习惯的改变和生活水平的提升,脑卒中的发病率越来越高,其已超过心脏病成为我国目前病亡的首要原因[16-20]。存活患者会出现各种不同程度的功能障碍,其中认知功能障碍是其中之一[21-25]。认知是人们认识和知晓事物过程的统称,包括感知、辨别、学习、计算、记忆、注意、理解、推理和判断等能力[26-30]。上述过程的某一方面或多方面损害,导致认知的效率降低或功能受损,即为认知功能障碍。认知功能障碍是脑卒中患者较为常见的后遗症之一,表现为记忆障碍、言语障碍、失认、失用、视空间障碍等,甚至痴呆[31-35]。有文献报道,约30%的脑卒中患者在发病后1 a内可出现不同程度的认知功能障碍,而这当中又有约1/3发展为痴呆[36-41],严重影响其生活和生存质量,给家庭和社会带来沉重的精神和经济负担。因此,对脑卒中患者的认知功能障碍进行早期干预以提高其生活和生存质量,并使之回归家庭和重返社会具有重要的现实意义。
有研究认为,中枢神经系统的功能及结构可塑性是很强的,经过一定强度的学习、多感觉刺激和系统
注:与头皮针治疗组比较,*P<0.05;与认知康复训练组比较,△P<0.05
图1 治疗后各组MoCA评分变化
Figure 1 Changes in MoCA scores of each group after treatment
表1 治疗后3个月各组韦氏评分疗效比较 [n(%)]
Table 1 Comparison of the efficacy of Wechsler scores in each group 3 months after treatment [n(%)]
| 组别 |
n |
显效 |
有效 |
无效 |
总有效 |
| 对照组 |
30 |
16 (53.33) |
4 (13.33) |
10 (33.33) |
20 (67.76) |
| 头皮针治疗组 |
30 |
22 (73.33) |
5 (16.67) |
3 (10.00) |
27 (90.00) |
| 认知康复训练组 |
30 |
23 (76.67) |
4 (13.33) |
3 (10.00) |
27 (90.00) |
| 联合治疗组 |
30 |
24 (80.00) |
5 (16.67) |
1 (3.33) |
29 (96.67)* |
注:与对照组相比,*P<0.05
训练后,大脑半球受损的某一脑区的功能可由附近未受损害的区域替代,并最终促进神经功能部分或完全恢复[42]。这可能是由于急性卒中后病灶周围水肿可逐渐缓解和侧支循环形成,使脑受损区的功能得到不同程度的恢复所致[43-44]。国内有学者研究认为,头针结合认知康复训练是众多针刺综合疗法中最有优势的,因针刺有调节突触可塑性,抑制炎症反应,减少细胞凋亡,增加大脑血流量等功能,进而可对认知功能进行整体调节,而认知康复训练通过针对性的训练和再学习刺激,可有效提高患者的认知功能,针刺与认知康复训练联合应用可产生协同效应,在促进神经系统自身重塑的基础上,促进实现神经整体网络的重塑及脑功能重组,从而促进神经功能的恢复,进而有效地提高脑卒中后认知障碍患者的认知功能[45-48]。
本研究发现,单纯给予神经内科药物对症治疗和常规康复训练的对照组MoCA评分治疗1个月、3个月、6个月后虽呈缓慢上升之势,但与前一个阶段的评分比较,差异无统计学意义(P>0.05),这可能是卒中后患者的自然康复过程的一个体现。头皮针治疗组、认知康复训练组和联合治疗组治疗1个月、3个月、6个月后每个阶段的评分均较前一个阶段有明显提高(P<0.05);治疗后3个月及6个月联合治疗组MoCA评分相对于单纯头皮针治疗组和单纯认知康复训练组明显升高(P<0.05)。另外,相对于对照组,治疗后3个月3组韦氏评分均有显著提升(P<0.05)。说明通过系统的认知训练和多感觉刺激,如头皮针等刺激,可通过调节突触的可塑性和减少神经细胞的凋亡等而使受损的脑认知功能区功能部分恢复,或被邻近正常脑区替代从而恢复功能,与前述国内外学者的研究一致。
认知康复训练结合头皮针治疗能有效提高脑卒中后认知障碍患者的认知功能,可使患者尽早回归家庭和重返社会,减轻了家庭的经济和精神负担,对患者个人及其家庭以及社会都有重要意义。
4 参考文献
[1] DUARTE-GARCA A,ROMERO-DAZ J,JUÁREZ S,et al.Disease activity,autoantibodies,and inflammatory molecules in serum and cerebrospinal fluid of patients with Systemic Lupus Erythematosus and Cognitive Dysfunction[J].PLoS One,2018,13(5):e0196487.
[2] KALARIA R N,AKINYEMI R,IHARA M.Stroke injury,cognitive impairment and vascular dementia[J].Biochim Biophys Acta,2016,1862(5):915-925.doi:10.1016/j.bbadis.2016.01.015
[3] PENG C Y,CHEN Y C,CUI Y,et al.Regional Coherence Alterations Revealed by Resting-State fMRI in Post-Stroke Patients with Cognitive Dysfunction[J].PLoS One,2016,11(7):e0159574.doi:10.1371/journal.pone.0159574
[4] 张辉,赵丽娜.老年急性脑梗死患者认知功能障碍分析及治疗研究[J].中国实用神经疾病杂志,2016,19(21):48-50.
[5] MIJAJLOVIC M D,PAVLOVIC A,BRAININ M,et al.Post-stroke dementia-a comprehensive review[J].BMC Med,2017,15:11.doi:10.1186/s12916-017-0779-7.
[6] GOTTESMAN R F,HILLIS A E.Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke[J].Lancet Neurol,2010,9(9):895-905.doi:10.1016/S1474-4422(10)70164-2.
[7] GEIGER M,BONNYAUD C,FERY Y A,et al.Evaluating the Effect of Cognitive Dysfunction on Mental Imagery in Patients with Stroke Using Temporal Congruence and the Imagined ‘Timed Up and Go’ Test (iTUG)[J].PLoS One,2017,12(1):e0170400.doi:10.1371/journal.pone.0170400.
[8] ZULKIFLY M F M,GHAZALI S E,DIN N C,et al.A Review of Risk Factors for Cognitive Impairment in Stroke Survivors[J].Sci World J,2016,2016:3456943.doi:10.1155/2016/3456943.
[9] IGNATOWSKI T A,SPENGLER R N,DHANDAPANI K M,et al.Perispinal Etanercept for Post-Stroke Neurological and Cognitive Dysfunction:Scientific Rationale and Current Evidence[J].CNS Drugs,2014,28(8):679-697.doi:10.1007/s40263-014-0174-2.
[10] SARFO F S,AKASSI J,ADAMU S,et al.Burden and Predictors of Post-Stroke Cognitive Impairment in a Sample of Ghanaian Stroke Survivors[J].J Stroke Cerebrovasc Dis,2017,26(11):2553-2562.doi:10.1016/j.jstrokecerebrovasdis.2017.05.041.
[11] 毛彦明,李玉成.尼麦角林联合奥拉西坦治疗脑卒中后血管性认知功能障碍[J].中国实用神经疾病杂志,2017,20(17):31-33.
[12] AKINYEMI R O,FIRBANK M,OGBOLE G I,et al.Medial temporal lobe atrophy,white matter hyperintensities and cognitive impairment among Nigerian African stroke survivors[J].BMC Res Notes,2015,8:625.doi:10.1186/s13104-015-1552-7.
[13] LEVINE D A,GALECKI A T,LANGA K M,et al.Trajectory of Cognitive Decline after Incident Stroke[J].JAMA,2015,314(1):41-51.doi:10.1001/jama.2015.6968.
[14] LI X T,YUAN J L,YANG L,et al.The significant effects of cerebral microbleeds on cognitive dysfun-ction:An updated meta-analysis[J].PLoS One,2017,12(9):e0185145.doi:10.1371/journal.pone.0185145.
[15] PAN C W,WANG X Z,MA Q H,et al.Cognitive dysfunction and health-related quality of life among older Chinese[J].Sci Rep,2015,5:17301.doi:10.1038/srep17301.
[16] BORDET R,IHL R,KORCZYN A D,et al.Towards the concept of disease-modifier in post-stroke or vascular cognitive impairment:a consensus report[J].BMC Med,2017,15:107.doi:10.1186/s12916-017-0869-6.
[17] NUSRAT L,LIVINGSTON-THOMAS J M,RAGUTHEVAN V,et al.Cyclosporin A-Mediated Activation of Endogenous Neural Precursor Cells Promotes Cognitive Recovery in a Mouse Model of Stroke[J].Front Aging Neurosci,2018,10:93.doi:10.3389/fnagi.2018.00093.
[18] 朱晓琳.老年患者口腔颌面外科术后认知功能障碍相关因素分析[J].中国实用神经疾病杂志,2017,20(4):72-73;144.
[19] NASREDDINE Z S,PHILLIPS N A,BEDIRIAN V,et al.The Montreal Cognitive Assessment,MoCA a brief screening tool for mild cognitive impairment[J].J Am Geriatr Soc,2005,53(4):695-699.
[20] JODOIN M,ROULEAU D,LARSON-DUPUIS C,et al.The clinical utility of repetitive transcranial magnetic stimulation in reducing the risks of transitioning from acute to chronic pain in traumatically injured patients[J].Prog Neuropsychopharmacol Biol Psychiatry,2018,87(Pt B):322-331.
[21] MORETTI D V,PATERNICO D,BINETTI G,et al.EEG markers are associated to gray matter changes in thalamus and basal ganglia in subjects with mild cognitive impairment[J].Neuroimage,2012,60(1):489-496.
[22] GORELICK P B,FURIE K L,IADECOLA C,et al.Defining Optimal Brain Health in Adults:A Presidential Advisory From the American Heart Association/American Stroke Association[J].Stroke,2017,48(10):e284-e303.
[23] FARACO G,SUGIYAMA Y,LANE D,et al.Perivascular macrophages mediate the neurovascular and cognitive dysfunction associated with hypertension[J].J Clin Invest,2016,126(12):4674-4689.doi:10.1172/JCI86950.
[24] XUAN S U X,WU Z Q,MAI F Y,et al.‘Governor vessel-unblocking and mind-regulating’ acupuncture therapy ameliorates cognitive dysfunction in a rat model of middle cerebral artery occlusion[J].Int J Mol Med,2019,43(1):221-232.doi:10.3892/ijmm.2018.3981.
[25] TADIC M,CUSPIDI C,HERING D.Hypertension and cognitive dysfunction in elderly:blood pressure management for this global burden[J].BMC Cardiovasc Disord,2016,16:208.doi:10.1186/s12872-016-0386-0.
[26] YANG S L,YE H C,HUANG J,et al.The synergistic effect of acupuncture and computer-based cognitive training on post-stroke cognitive dysfunction:a study protocol for a randomized controlled trial of 2×2 factorial design[J].BMC Complement Altern Med,2014,14:290.doi:10.1186/1472-6882-14-290.
[27] WANG F,ZOU Z R,YUAN D,et al.Correlation between serum S100β protein levels and cognitive dysfunction in patients with cerebral small vessel disease:a case-control study[J].Biosci Rep,2017,37(2):BSR20160446.doi:10.1042/BSR20160446.
[28] CHEN A Q,AKINYEMI R O,HASE Y,et al.Frontal white matter hyperintensities,clasmatodendrosis and gliovascular abnormalities in ageing and post-stroke dementia[J].Brain,2016,139(1):242-258.doi:10.1093/brain/awv328.
[29] COCO D L,LOPEZ G,CORRAO S.Cognitive impairment and stroke in elderly patients[J].Vasc Health Risk Manag,2016,12:105-116.doi:10.2147/VHRM.S75306.
[30] BERGER M,NADLER J,BROWNDYKE J,et al.Postoperative Cognitive Dysfunction:Minding the Gaps in our Knowledge of A Common Postoperative Complication in the Elderly[J].Anesthesiol Clin,2015,33(3):517-550.doi:10.1016/j.anclin.2015.05.008.
[31] LEVINE D A,KABETO M,LANGA K M,et al.Does Stroke Contribute to Racial Differences in Cognitive Decline?[J].Stroke,2015,46(7):1897-1902.doi:10.1161/STROKEAHA.114.008156.
[32] MELLON L,BREWER L,HALL P,et al.Cognitive impairment six months after ischaemic stroke:a profile from the ASPIRE-S study[J].BMC Neurol,2015,15:31.doi:10.1186/s12883-015-0288-2.
[33] YU H,DONG R,LU Y Y,et al. Short-Term Postope-rative Cognitive Dysfunction and Inflammatory Re-sponse in Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy:A Pilot Study[J].Mediators Inflamm,2017,2017:3605350.doi:10.1155/2017/3605350.
[34] SETO S W,YANG G Y,KIAT H,et al.Diabetes Me-llitus,Cognitive Impairment,and Traditional Chinese Medicine[J].Int J Endocrinol,2015,2015:810439.doi:10.1155/2015/810439.
[35] ZUO L J,LI Z X,ZHU R Y,et al. The Relationship between Cerebral White Matter Integrity and Cognitive Function in Mild Stroke with Basal Ganglia Region Infarcts[J].Sci Rep,2018,8:8422.doi:10.1038/s41598-018-26316-5.
[36] DOYLE K P,BUCKWALTER M S.Does B lymphocyte-mediated autoimmunity contribute to post-stroke dementia?[J].Brain Behav Immun,2017,64:1-8.doi:10.1016/j.bbi.2016.08.009.
[37] MANCUSO M,DEMEYERE N,ABBRUZZESE L,et al.Using the Oxford Cognitive Screen to Detect Cognitive Impairment in Stroke Patients:A Comparison with the Mini-Mental State Examination[J].Front Neurol,2018,9:101.doi:10.3389/fneur.2018.00101.
[38] HARDIGAN T,WARD R,ERGUL A.Cerebrovascular Complications of Diabetes:Focus on Cognitive Dysfunction[J].Clin Sci (Lond),2016,130(20):1807-1822.doi:10.1042/CS20160397.
[39] FU X J,LU Z N,WANG Y,et al.A Clinical Research Study of Cognitive Dysfunction and Affective Impairment after Isolated Brainstem Stroke[J].Front Aging Neurosci,2017,9:400.doi:10.3389/fnagi.2017.00400.
[40] SINGH-MANOUX A,FAYOSSE A,SABIA S,et al.Atrial fibrillation as a risk factor for cognitive decline and dementia[J].Eur Heart J,2017,38(34):2612-2618.doi:10.1093/eurheartj/ehx208.
[41] GILLETT S R,THACKER E L,LETTER A J,et al.Correlates of Incident Cognitive Impairment in the REasons for Geographic and Racial Differences in Stroke (REGARDS) Study[J].Clin Neuropsychol,2015,29(4):466-486.doi:10.1080/13854046.2015.1042524.
[42] RAJAN K B,AGGARWAL N T,SCHNEIDER J A,et al.Role of APOEε4 Allele and Incident Stroke on Cognitive Decline and Mortality[J].Alzheimer Dis Assoc Disord,2016,30(4):318-323.doi:10.1097/WAD.0000000000000173.
[43] ZUO L J,DONG Y H,ZHU R Y,et al.Screening for cognitive impairment with the Montreal Cognitive Assessment in Chinese patients with acute mild stroke and transient ischaemic attack:a validation study[J].BMJ Open,2016,6(7):e011310.doi:10.1136/bmjopen-2016-011310.
[44] CHEN X L,DUAN L H,HAN Y F,et al.Predictors for vascular cognitive impairment in stroke patients[J].BMC Neurol,2016,16:115.doi:10.1186/s12883-016-0638-8.
[45] MRKOBRADA M,CHAN M T V,COWAN D,et al.Rationale and design for the detection and neurological impact of cerebrovascular events in non-cardiac surgery patients cohort evaluation (NeuroVISION) study:a prospective international cohortstudy[J].BMJ Open,2018,8(7):e021521.doi:10.1136/bmjopen-2018-021521.
[46] DOYLE K P,QUACH L N,SOL M,et al.B-Lymphocyte-Mediated Delayed Cognitive Impairment following Stroke[J].J Neurosci,2015,35(5):2133-2145.doi:10.1523/JNEUROSCI.4098-14.2015.
[47] ZHOU J,LI J,ROSENBAUM D M,et al.The prolyl 4-hydroxylase inhibitor GSK360A decreases post-stroke brain injury and sensory,motor,and cognitive behavioral deficits[J].PLoS One,2017,12(9):e0184049.doi:10.1371/journal.pone.0184049.
[48] SASHIKA H,TAKADA K,KIKUCHI N.Rehabilita-tion needs and participation restriction in patients with cognitive disorder in the chronic phase of traumatic brain injury[J].Medicine (Baltimore),2017,96(4):e5968.doi:10.1097/MD.0000000000005968.
(收稿2018-08-26 修回2018-10-06)
本文责编:夏保军
本文引用信息:车文生,蔡琛.认知康复训练结合头皮针治疗脑卒中后认知功能障碍的疗效观察[J].中国实用神经疾病杂志,2018,21(24):2719-2724.DOI:10.12083/SYSJ.2018.24.567
Reference information:CHE Wensheng,CAI Chen.Effect of cognitive rehabilitation training combined with scalp acupuncture on cognitive dysfunction after stroke[J].Chinese Journal of Practical Nervous Diseases,2018,21(24):2719-2724.DOI:10.12083/SYSJ.2018.24.567