目的 探讨软通道微创介入治疗老年高血压脑出血(HICH)的疗效。方法 将黄河中心医院神经内科和重症医学科2014-01—2016-12收治的124例老年HICH患者随机分为研究组和对照组各62例。对照组采用硬通道微创术治疗,研究组采用软通道微创术介入治疗。观察2组临床疗效、术后并发症发生情况及生存质量(QOL)评分。结果 研究组治疗总有效率略高于对照组,但2组比较差异无统计学意义(P>0.05);研究组术后并发症发生率明显低于对照组,差异有统计学意义(P<0.01);术后随访6个月,研究组生存质量评分高于对照组,差异有统计学意义(P<0.05)。结论 硬通道微创与软通道微创介入治疗老年HICH的效果相当,但软通道微创介入治疗的并发症发生率低,在减少组织损伤、恢复神经功能、改善患者生活质量方面更具优势。
软通道微创介入治疗老年高血压脑出血临床观察
崔 琳
黄河中心医院,河南 郑州 450000
作者简介:崔琳,Email:799324764@qq.com
【摘要】 目的 探讨软通道微创介入治疗老年高血压脑出血(HICH)的疗效。方法 将黄河中心医院神经内科和重症医学科2014-01—2016-12收治的124例老年HICH患者随机分为研究组和对照组各62例。对照组采用硬通道微创术治疗,研究组采用软通道微创术介入治疗。观察2组临床疗效、术后并发症发生情况及生存质量(QOL)评分。结果 研究组治疗总有效率略高于对照组,但2组比较差异无统计学意义(P>0.05);研究组术后并发症发生率明显低于对照组,差异有统计学意义(P<0.01);术后随访6个月,研究组生存质量评分高于对照组,差异有统计学意义(P<0.05)。结论 硬通道微创与软通道微创介入治疗老年HICH的效果相当,但软通道微创介入治疗的并发症发生率低,在减少组织损伤、恢复神经功能、改善患者生活质量方面更具优势。
【关键词】 高血压脑出血;微创介入;软通道;硬通道;老年;生存质量;预后
【中图分类号】 R743.34 【文献标识码】 A 【文章编号】 1673-5110(2019)02-0197-05 DOI:10.12083/SYSJ.2019.02.038
Clinical observation of soft channel minimally invasive in the treatment of hypertensive intracerebral hemorrhage in the elderly
CUI Lin
Huanghe Central Hospital,Zhengzhou 450000,China
【Abstract】 Objective To research the effect of soft channel minimally invasive treatment of hypertensive intracerebral hemorrhage (HICH) in the elderly.Methods In this study,124 patients with HICH in the Department of Neurology and Intensive Care Unit(ICU)of Huanghe Central Hospital from January 2014 to December 2016 were randomly divided into the study group and the control group,each with 62 cases.The control group was treated by hard channel minimally invasive surgery,and the study group was treated with soft channel minimally invasive interventional therapy.The clinical curative effect,postoperative complications and the scores of quality of life (QOL) in both groups were compared.Results The total effective rate in the study group was slightly higher than that in the control group,there was no significant difference between the two groups(P>0.05).The incidence of postoperative complications in the study group was significantly lower than that in the control group,there was a significant difference (P<0.05).After 6 months of follow-up,the survival quality score of the study group was higher than that in the control group,there was a significant difference (P<0.05).Conclusion Hard channel of minimally invasive treatment and soft channel of minimally invasive interventional treatment have equal effect in treatment of HICH in the elderly,but the soft channel of minimally invasive interventional treatment has less complications,and has advantages on decreasing tissue damage,restoring nerve function,reducing the incidence of complications,and improving the quality of life,which is worth of clinical promotion.
【Key words】 Hypertensive intracerebral hemorrhage;Minimally invasive;Soft channel;Hard channel;Elderly;Life quality;Prognosis
由于不合理的生活习惯导致高血压的发病率逐年提高[1-3]。高血压脑出血(hypertensive intracere-bral hemorrhage,HICH)是脑血管急症之一,是继发于高血压或原发于脑实质内的一种出血性疾病[4-6],主要指脑内动脉、静脉或毛细血管在长期高血压状态下破裂并引起的脑实质内出血,病情危急,进展快,具有较高的致残率和病死率[3]。高血压脑出血临床治疗的时效性要求很高,单纯内科保守治疗效果欠佳,手术治疗可有效清除血肿。高血压脑出血对颅脑组织造成直接损伤外,血肿在颅内引起继发性炎症反应,从而导致脑组织水肿,水肿可对颅脑组织和神经造成持续性损伤,影响预后。颅内微创血肿清除术是目前治疗脑出血的主要方法[7-8]。临床治疗中硬通道及软通道微创术均较常见,但对其应用价值的争议仍较大[9-10]。
1 资料与方法
1.1 一般资料 选取黄河中心医院神经内科和重症医学科2014-01—2016-12收治的124例老年高血压脑出血,所有患者经临床症状、CT 或MRI、血尿常规、病史、实验室等检查证实为高血压脑出血[11]。纳入标准:(1)有高血压史;(2)年龄60岁以上;(3)出血量30~80 mL;(4)患者及家属接受手术治疗方式并签署知情同意书。排除标准:(1)其他原因引用的脑出血;(2)病情持续恶化,脑疝形成患者;(3)合并心、肺、肝、肾功能不全者;(4)近期服用过抗血小板药物或抗凝药物者;(5)患者或其家属不同意手术治疗。随机分为分为研究组和对照组各62例。研究组男30例,女32例;年龄60~80(68.2±6.9)岁;血肿量30~79 mL。对照组男32例,女30例;年龄61~80(68.8±7.6)岁;血肿量30.6~80.0 mL。2组一般资料比较差异均无统计学意义(P>0.05),具有可比性。
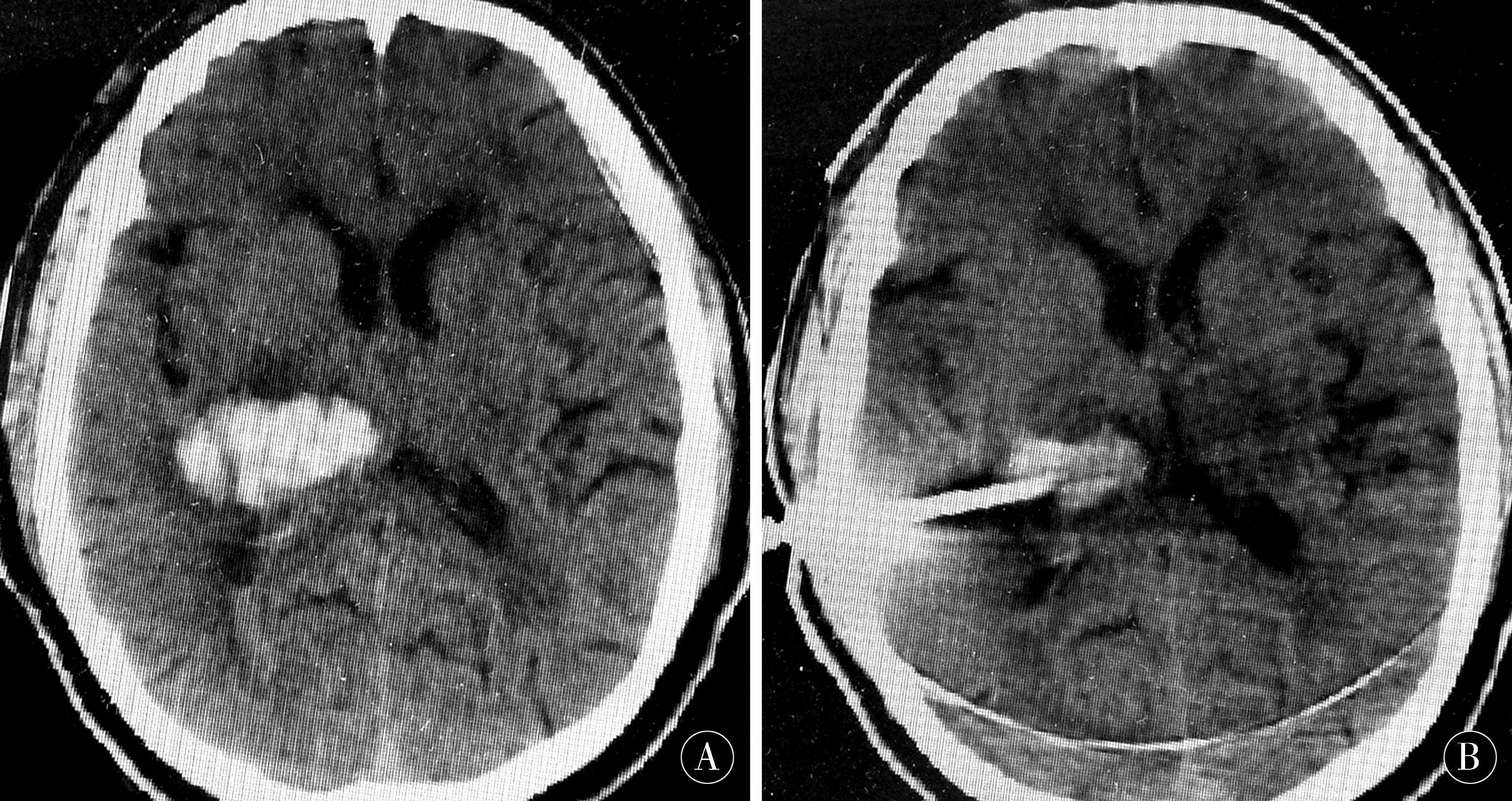
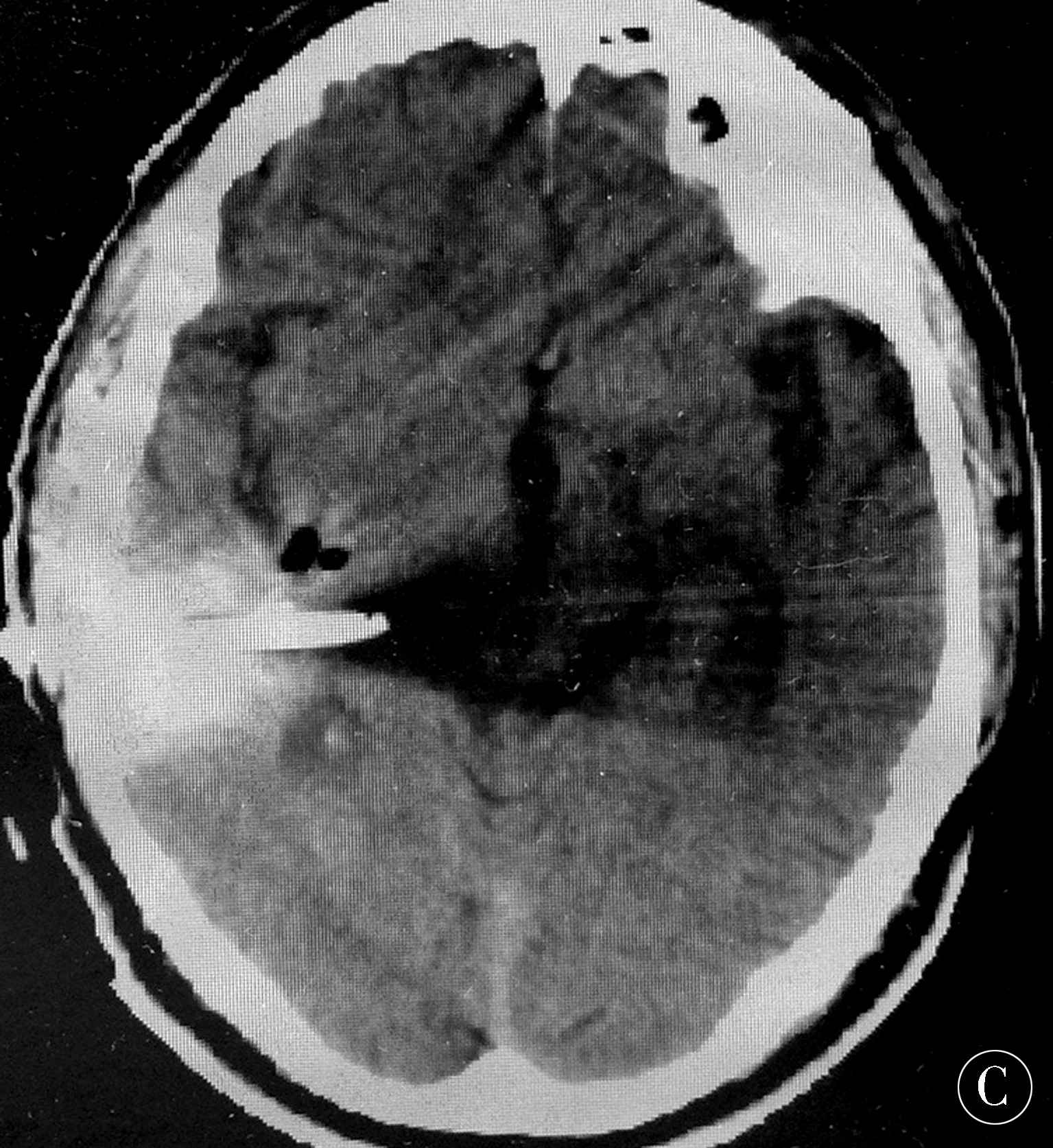
1.2 治疗方法 入院后采取常规脱水、降颅压、营养神经、改善脑循环、保护靶器官、抗感染、营养支持、维持内环境稳定等治疗方案。研究组采用软通道微创介入术,根据颅脑CT结果确定最大层面血肿中心为穿刺平面,确定血肿中心靶点和入颅途径;局部麻醉后,定向穿透颅骨及硬膜外血肿腔,导入软通道穿刺引流管,建立引流通道,并采用5 mL注射器抽吸血肿(对液态积血抽吸,注意适当速度),首次抽吸血肿量的30%~60%,血凝块难以吸出可留置引流管,注入生理盐水、尿激酶冲洗,术后每日分次将生理盐水稀释的5 mL尿激酶注入血肿腔,闭管2 h后打开,根据具体情况引流。术后1周内复查头颅CT,当血肿清除率>70%,无不适可拔管(图1)。
图1 A:术前右侧基底节区出血量38 mL;B:术中引流出血肿量18 mL;C:术后第3天复查,出血基本引流干净
Figure 1 A:The amount of bleeding in the right basal ganglia before surgery is 38 mL;B:The amount of bleeding in the operation is 18 mL;C:On the third day after surgery,the basic drainage is clean
对照组采取硬通道微创术治疗,定位方法与软通道微创介入相同。根据影像学检查结果确定穿刺点,麻醉后选择合适长度的一次性颅内血肿粉碎穿刺针固定在电钻上,穿过硬脑膜,进入血肿中心建立硬通道,缓慢负压抽吸血肿,根据复查CT结果,确立适当的液化周期并实施重复血肿抽吸,根据复查头颅结果,一般1周内无不适症状可拔除穿刺针[12-14]。
1.3 疗效评定 采用美国国立卫生院卒中量表(NHISS)评分和生存质量(QOL)评分(分值越高,生活质量越高)评价神经功能缺损程度和日常生活能力、生存质量。术后效果评定标准:NHISS减分≥91%,ADLⅠ级为基本痊愈;NHISS减分46%~90%,ADL≤Ⅲ级为显效;NHISS减分18%~46%,ADLⅣ级为有效;NHISS减分≤18%,ADLⅤ级均为无效[15-18]。总有效率=(基本痊愈+显效+有效)/总例数×100%。生存质量分级:生存质量满分为60分,51~60分为良好,41~50分为较好,31~40分为一般,21~30分为差,<20分为极差[19-22]。
1.4 统计学处理 应用SPSS 18.0 统计软件进行统计学分析,计量资料以均数±标准差(x±s)表示,组间比较采用t检验;计数资料以率或构成比表示,采用χ2检验。P<0.05为差异有统计学意义。
2 结果
2.1 术后疗效对比 研究组总有效率略高于对照组,但差异无统计学意义(χ2=6.04,P>0.05)。见表1。
2.2 术后并发症 研究组术后感染、再出血、颅内积气、软组织损伤等并发症的发生率明显低于对照组(χ2=20.52,P<0.01)。见表2。
2.3 NIHSS及QOL评分情况 术前2组NIHSS评分比较,差异无统计学意义(P>0.05),术后2组NIHSS评分均较术前显著降低,且研究组明显低于对照组(P<0.05);随访6个月,研究组QOL评分明显高于对照组(P<0.05)。见表3。
3 讨论
高血压脑出血是脑内细小动脉在长期高血压作用下发生玻璃样变性、纤维素样坏死,甚至形成微动脉瘤或夹层动脉瘤,血压骤然升高导致血管破裂出血,而患者血管本身无畸形、淀粉样病变、凝血障碍或血液系统疾病[23-25]。研究表明[19,26-28],高血压脑出血的颅内血肿作为脑出血病理生理改变的核心,可诱发多种生理变化及继发性损害,脑出血后会触发凝血级联反应,产生大量凝血酶,凝血酶具有神经毒性作用,加重脑损伤。对于老年高血压脑出血患者,传统的手术治疗效果不是很理想,易出现各种并发症[29-30]。近年来,微创介入治疗老年高血压脑出血逐步开展,具有损伤小、操作简便、对周围组织影响较小的优势,且术后并发症少,患者康复快,生存质量高。
表1 2组术后疗效比较 [n(%)]
Table 1 Comparison of postoperative efficacy between two groups [n(%)]
| 组别 |
n |
基本痊愈 |
显效 |
有效 |
无效 |
总有效率/% |
| 对照组 |
62 |
23(37.1) |
17(27.4) |
16(25.8) |
6(9.7) |
90.32 |
| 研究组 |
62 |
31(50.0) |
14(22.6) |
14(22.6) |
3(4.8) |
95.16 |
表2 2组术后并发症发生率比较 [n(%)]
Table 2 Comparison of the incidence of postoperative complications between the two groups [n(%)]
| 组别 |
n |
感染 |
再出血 |
颅内积气 |
软组织损伤 |
总发生 |
| 对照组 |
62 |
11(17.7) |
19(30.6) |
8(12.9) |
20(32.2) |
58(93.54) |
| 研究组 |
62 |
6(9.7) |
2(3.2) |
11(17.7) |
0 |
19(30.64) |
表3 2组NIHSS评分及术后QOL评分比较 (x±s,分)
Table 3 Comparison of NIHSS score and postoperative QOL score between two groups (x±s,分)
| 组别 |
n |
术前NIHSS评分 |
术后NIHSS评分 |
QOL评分 |
| 对照组 |
62 |
17.6±6.2 |
14.8±5.4 |
31.72±7.07 |
| 研究组 |
62 |
17.8±6.8 |
12.2±5.0 |
45.87±8.62 |
在微创介入治疗颅内血肿方面,有软通道和硬通道两种。本研究显示,两种方法治疗老年高血压脑出血的有效率无明显差别,但在并发症发生率和生存质量上,软通道较硬通道有明显优势。硬通道对血肿负压抽吸时管腔坚硬无塌陷,可将血肿快速清除,降低颅内压。但硬通道质地坚硬,无法根据血肿的变化调整抽吸方向,全方位旋转抽吸残留的血肿,对血肿外周围脑组织伤害较大。软通道微创介入术具有以下优点:(1)灵活性高:软通道颅内引流管质地柔软,引流管变形性良好,引流效果不受血肿腔缩小、变形影响,具有较高的操作灵活性,适用于颅内各部位血肿的手术治疗;(2)创伤小:材质柔软,兼容性好,消毒方便,进管时对脑组织及血管起分离作用,对脑组织造成的损伤较小;(3)软通道微创介入术操作简便、及时,清除颅内血肿安全有效,再出血及感染机会少,并发症少,住院时间短;(4)引流管的口径较大,抽吸血肿更彻底,且软管可根据脑组织复位进行移动,根据CT复查结果调整软管深度,对患者的损伤较小;(5)手术适用范围广,特别是适用于耐受性差的老年患者。软通道微创手术创伤小,患者恢复好,病死率低,安全有效。研究发现[28],软通道微创手术继发颅内感染较硬通道少,虽手术时间长,但安全性更高,有利于术后患者的康复。研究[26]认为,在临床治疗高血压脑出血患者的过程中,软通道微创术可以有效降低临床感染率,控制炎性指标,显著改善其应激状态,是治疗高血压脑出血的理想方式之一。高血压脑出血患者应用微创软通道穿刺引流的临床治疗效果明显,且可以使患者的日常生活以及生活能力显著提高。
心脑血管损伤时,CRP、同型半胱氨酸(Hcy)、BNP被大量分泌至血浆中,其与脑血管疾病的发生、发展密切有关,可作为脑血管病诊治的参考指标。本研究中2组疗效相当,是否与术后效果评定指标不够全面有关,还有待进一步研究。如将出血部位与CRP、Hcy、BNP等指标变化结合,进一步确定软通道与硬通道微创术对不同部位脑出血的疗效,相信会对今后脑出血微创术的发展有更进一步的指导意义。
4 参考文献
[1] GU B,ZHAO Y C,YANG Z W,et al.HindIII polymorphism in the lipoprotein lipase gene and hypertensive intracerebral hemorrhage in the Chinese Han population[J].J Stroke Cerebrovasc Dis,2014,23(6):1 275-1 281.
[2] HAN Y,SHENG K,SU M,et al.Local mild hypother-mia therapy as an augmentation strategy for minimally invasive surgery of hypertensive intracerebral hemorrhage:a meta-analysis of randomized clinical trials[J].Neuropsychiatr Dis Treat,2016,13:41-49.
[3] XU X,ZHENG Y,CHEN X,et al.Comparison of endoscopic evacuation,stereotactic aspiration and craniotomy for the treatment of supratentorial hypertensive intracerebral haemorrhage:study protocol for a randomised controlled trial[J].Trials,2017,18(1):296.
[4] WANG W,ZHOU N,WANG C.Minimally Invasive Surgery for Patients with Hypertensive Intracerebral Hemorrhage with Large Hematoma Volume:A Retrospective Study[J].World Neurosurg,2017,105:348-358.
[5] CHARIDIMOU A,PASI M,FIORELI M,et al.Leukoaraiosis,cerebral hemorrhage,and outcome after intravenous thrombolysis for acute ischemic stroke:a meta analysis(vl)[J].Stroke,2016,47(9):2 364-2 372.
[6] UZUNOV K.The transcortical frontal approach in putaminal hypertensive intracerebral haematomas[J].Khirurgiia (Sofiia),2009(2/3):45-48.
[7] YANG Q,ZHUANG X,PENG P,et al.Relationship of plasma matrix metalloproteinase-9 and hematoma in acute hypertensive cerebral hemorrhage[J].Int J Nerosci,2016,126(3):313-248.
[8] MCCOURT R,GOULD B,GIOIA L,et al.Cerebral perfusion and blood pressure do not affect perihematoma edema growth in acute intracerebral hemorrhage[J].Stroke,2014,45(5):1 292-1 298.
[9] YANG L J,CUI J L,WU T M,et al.Sequential therapy for non-thalamus supratentorial hypertensive intracerebral hemorrhages[J].Eur Rev Med Pharmacol Sci,2014,18(23):3 653-3 658.
[10] WANG G Q,LI S Q,HUANG Y H,et al.Can minimally invasive puncture and drainage for hypertensive spontaneous Basal Ganglia intracerebral hemorrhage improve patient outcome:a prospective non-randomized comparative study[J].Mil Med Res,2014,1:10.
[11] GUSHCHA A O,SEMENOV M S,LEPSVERIDZE L T.Experience of endoscopic removal of hypertensive intracerebral hemorrhage[J].Zh Vopr Neirokhir Im N N Burdenko,2015,79(6):71-76.
[12] ZHAO J Z,ZHOU D B,ZHOU L F,et al.The efficacy of three different approaches in treatment of hypertensive intracerebral hemorrhage:a multi-center single-blind study of 2464 patients[J].Zhonghua Yi Xue Za Zhi,2005,85(32):2 238-2 242.
[13] WANG D J,WANG S,ZHAO Y L,et al.Multianalysis of short-term prognostic factors in surgical practices for hypertensive intracerebral hemorrhage[J].Zhonghua Yi Xue Za Zhi,2005,85(44):3 118-3 122.
[14] LEI C,WU B,LIU M,et al.Differences Between Vascular Structural Abnormality and Hypertensive Intracerebral Hemorrhage[J].J Stroke Cerebrovasc Dis,2015,24(8):1 811-1 816.
[15] GANG Y,SHAO G.Clinical effect of minimally invasive intracranial hematoma in treating hypertensive cerebral hemorrhage[J].Pak J Med Sci,2016,32(3):677-681.
[16] TIAN D Z,WEI W,DONG Y J.Influence of COL1A2 gene variants on the incidence of hypertensive intracerebral hemorrhage in a Chinese population[J].Genet Mol Res,2016,15(1).DOI:10.4238/gmr.15017369.
[17] AGMAZOV M K,BERSNEV V P,IVANOVA N E,et al.Minimally invasive surgery of patients with hypertensive intracerebral bleedings[J].Vestn Khir Im I I Grek,2009,168(2):78-82.
[18] DING D,PRZYBYLOWSKI C J,STARKE R M,et al.A minimally invasive anterior skull base approach for evacuation of a basal ganglia hemorrhage[J].J Clin Neurosci,2015,22(11):1 816-1 819.
[19] MOUSSA W M,KHEDR W.Decompressive craniectomy and expansive duraplasty with evacuation of hyperten-sive intracerebral hematoma,a randomized controlled trial[J].Neurosurg Rev,2017,40(1):115-127.
[20] CHEN Q H,LIN D,YU Q G,et al.Efficacy of lumbar cistern drainage combined with intrathecal antibiotherapy for the treatment of ventriculo-subarachnoid infections following surgery for hypertensive intracerebral hemorrhage[J].Neurochirurgie,2017,63(1):13-16.
[21] ZHAO Y N,CHEN X L.Endoscopic treatment of hypertensive intracerebral hemorrhage:A technical review[J].Chronic Dis Transl Med,2016,2(3):140-146.
[22] SARIBEKIAN A S,PONOMAREV V A,POLIAKOVA L N,et al.Mortality after surgical treatment of patients with hypertensive intracerebral hematomas[J].Zh Vopr Neirokhir Im N N Burdenko,2009(1):3-11.
[23] ZHAO Z,WANG H,LI Z,et al.Assessment of the effect of short-term factors on surgical treatments for hypertensive intracerebral haemorrhage[J].Clin Neurol Neurosurg,2016,150:67-71.
[24] YANG Z,HONG B,JIA Z,et al.Treatment of supratentorial spontaneous intracerebral hemorrhage using image-guided minimally invasive surgery:Initial experiences of a flat detector CT-based puncture planning and navigation system in the angiographic suite[J].AJNR Am J Neuroradiol,2014,35(11):2 170-2 175.
[25] WU G,ZHONG W.Effect of minimally invasive surgery for cerebral hematoma evacuation in different stages on motor evoked potential and thrombin in dog model of intracranial hemorrhage[J].Neurol Res,2010,32(2):127-133.
[26] YANG G,SHAO G.Clinical effect of minimally invasive intracranial hematoma in treating hypertensive cerebral hemorrhage[J].Pak J Med Sci,2016,32(3):677-681.
[27] YADAV Y R,YADAV S,SHEREKAR S,et al.A new minimally invasive tubular brain retractor system for surgery of deep intracerebral hematoma[J].Neurol India,2011,59(1):74-77.
[28] QIU Y,LIN Y,TIAN X,et al.Hypertensive intracranial hematomas:endoscopic-assisted keyhole evacuation and application of patent viewing dissector[J].Chin Med J (Engl),2003,116(2):195-199.
[29] LI F,CHEN Q X,XIANG S G,et al.N-Terminal Pro-Brain Natriuretic Peptide Concentrations After Hypertensive Intracerebral Hemorrhage:Relationship With Hematoma Size,Hyponatremia,and Intracranial Pressure[J].J Intensive Care Med,2018,33(12):663-670.
(收稿2018-05-11)
本文责编:夏保军
本文引用信息:崔琳.软通道微创介入治疗老年高血压脑出血临床观察[J].中国实用神经疾病杂志,2019,22(2):197-201.DOI:10.12083/SYSJ.2019.02.038
Reference information:CUI Lin.Clinical observation of soft channel minimally invasive in the treatment of hypertensive intracerebral hemorrhage in the elderly[J].Chinese Journal of Practical Nervous Diseases,2019,22(2):197-201.DOI:10.12083/SYSJ.2019.02.038